Anda mungkin juga menyukai
- Unit 2 MCB Key PDFDokumen19 halamanUnit 2 MCB Key PDFDafne Fertig88% (32)
- API-650 Design Procedure ExampleDokumen21 halamanAPI-650 Design Procedure Examplegdwvcd93% (14)
- New Model For Predicting Thermal Radiation From Flares and High Pressure Jet Fires For Hydrogen and SyngasDokumen15 halamanNew Model For Predicting Thermal Radiation From Flares and High Pressure Jet Fires For Hydrogen and Syngasthlim19078656Belum ada peringkat
- E-Studio 205L, 255, 305, 355, 455 MFP Service HandbookDokumen732 halamanE-Studio 205L, 255, 305, 355, 455 MFP Service HandbookAnonymous gn8qxx66% (35)
- Manual Prevention An Control of Lost Cir PDFDokumen222 halamanManual Prevention An Control of Lost Cir PDFAna Maria TovarBelum ada peringkat
- Medicinal Chemistry 1 - Full VersionDokumen199 halamanMedicinal Chemistry 1 - Full Versionsaddamixo100% (2)
- Absorption and Extraction of ToxinDokumen22 halamanAbsorption and Extraction of Toxinabhishekranjan090202Belum ada peringkat
- Ulangkaji Exam MDM DDokumen10 halamanUlangkaji Exam MDM DAsyraf RefdinBelum ada peringkat
- Toxicology L3Dokumen24 halamanToxicology L3MA 09Belum ada peringkat
- Pharmaco KineticsDokumen69 halamanPharmaco KineticsSristeeBelum ada peringkat
- Pharmacokinetics - 1Dokumen41 halamanPharmacokinetics - 1SristeeBelum ada peringkat
- Chapter III Pharmacokinetics: Durge Raj GhalanDokumen64 halamanChapter III Pharmacokinetics: Durge Raj GhalanDurge Raj Ghalan100% (3)
- Drug Absorption: - Absorption Is The Process byDokumen57 halamanDrug Absorption: - Absorption Is The Process byccccccc1Belum ada peringkat
- Cell MembraneDokumen41 halamanCell MembraneBima ArisandiBelum ada peringkat
- 4 - Pharmacokinetics 2Dokumen30 halaman4 - Pharmacokinetics 2YEOH WANYUBelum ada peringkat
- General Pharmacology (1-7)Dokumen7 halamanGeneral Pharmacology (1-7)LotfyAdel100% (1)
- Absorpsi ObatDokumen30 halamanAbsorpsi ObatdanielBelum ada peringkat
- Absorption and Distribution - 2023Dokumen34 halamanAbsorption and Distribution - 2023Rhythm BhardwajBelum ada peringkat
- Kuliah FarmakologiDokumen74 halamanKuliah FarmakologiHanifBelum ada peringkat
- Thomas L. Pazdernik, Laszlo Kerecsen-Rapid Review Pharmacology, 3rd Edition-Mosby (2010)Dokumen784 halamanThomas L. Pazdernik, Laszlo Kerecsen-Rapid Review Pharmacology, 3rd Edition-Mosby (2010)dtech2Belum ada peringkat
- Cell Bio Chapter 5Dokumen23 halamanCell Bio Chapter 5busachala517Belum ada peringkat
- AbsorptionDokumen42 halamanAbsorptionPrathamesh PatilBelum ada peringkat
- Uc PDFDokumen6 halamanUc PDFPenBelum ada peringkat
- Absorption of DrugsDokumen41 halamanAbsorption of DrugsSibtain100% (2)
- Handbook of VeterinaryDokumen4 halamanHandbook of VeterinarySyifa ZataliniBelum ada peringkat
- AbsorptionDokumen61 halamanAbsorptionGreenBelum ada peringkat
- Neeraj Assignment PDFDokumen68 halamanNeeraj Assignment PDFNeeraj GautamBelum ada peringkat
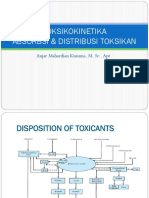
- Disposition of ToxicantsDokumen102 halamanDisposition of ToxicantsApoorvi JainBelum ada peringkat
- Scan 0003Dokumen7 halamanScan 0003abtkkBelum ada peringkat
- Physiology Study MaterialsDokumen68 halamanPhysiology Study MaterialsBruntBelum ada peringkat
- UNIT 1 Introduction To BiopharmaceuticsDokumen208 halamanUNIT 1 Introduction To BiopharmaceuticsMamta Pant100% (5)
- Pharmaceutical Chemistry I (Phcm571) Lecture 3, Drug Metabolism IDokumen42 halamanPharmaceutical Chemistry I (Phcm571) Lecture 3, Drug Metabolism IMirette AshrafBelum ada peringkat
- Ico Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanDokumen34 halamanIco Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanMelkamu AyeBelum ada peringkat
- Absorption and Distribution of Toxicants - L4Dokumen3 halamanAbsorption and Distribution of Toxicants - L4prasad sanjayaBelum ada peringkat
- Biopharmaceutics AbsorptionDokumen49 halamanBiopharmaceutics AbsorptionSaul Antonio Montoya SerranoBelum ada peringkat
- AbsorptionDokumen42 halamanAbsorptionPrathamesh PatilBelum ada peringkat
- Transport Across The Cell MembraneDokumen11 halamanTransport Across The Cell MembraneMae Balubar PolidoBelum ada peringkat
- Absorption, Distribution, Metabolism and Excretion: Prof. Ian Hughes, 9.83, I.e.hughes@leeds - Ac.ukDokumen176 halamanAbsorption, Distribution, Metabolism and Excretion: Prof. Ian Hughes, 9.83, I.e.hughes@leeds - Ac.ukdipti_srivBelum ada peringkat
- PHARMACOKINETICSDokumen55 halamanPHARMACOKINETICSnezifzenu2023Belum ada peringkat
- The Ladmer SystemDokumen12 halamanThe Ladmer Systemkriss WongBelum ada peringkat
- Welcome To Our PresentationDokumen29 halamanWelcome To Our PresentationSufia SuptyBelum ada peringkat
- Biopharmaceutics: Institute of Pharmaceutical ResearchDokumen31 halamanBiopharmaceutics: Institute of Pharmaceutical ResearchNaman SharmaBelum ada peringkat
- Principle of Drug Action 2021Dokumen31 halamanPrinciple of Drug Action 2021cindy8127Belum ada peringkat
- Drug Absorption MechanismDokumen20 halamanDrug Absorption MechanismhabibieBelum ada peringkat
- 2 Dan 3. Metabolisme XenobiotikDokumen137 halaman2 Dan 3. Metabolisme Xenobiotikdevi enjelikaBelum ada peringkat
- BIOPHARMACEUTICS and PHARMACOKINETICSDokumen20 halamanBIOPHARMACEUTICS and PHARMACOKINETICSPrincess Rose Gamboa100% (1)
- Lecture No. 4 (PHARMACOKINETICS - Mechanism of Drug Transport Processes)Dokumen9 halamanLecture No. 4 (PHARMACOKINETICS - Mechanism of Drug Transport Processes)tejasbhukal567Belum ada peringkat
- Grup 4 Passage of Drugs Across Biology MembraneDokumen24 halamanGrup 4 Passage of Drugs Across Biology MembraneIndiy Heny SaLindriBelum ada peringkat
- Major ElectrolytesDokumen4 halamanMajor Electrolytes6k8rtwgpksBelum ada peringkat
- Chapter 5Dokumen20 halamanChapter 5skywalkerBelum ada peringkat
- Drug Transport Across Cell Membrane: Dr. Salman H. RizviDokumen67 halamanDrug Transport Across Cell Membrane: Dr. Salman H. RizviIrum RafeeqBelum ada peringkat
- Biolab2 Report FinalDokumen14 halamanBiolab2 Report FinalKriztle de los ReyesBelum ada peringkat
- Chapter 3: Cell Structures and Their FunctionsDokumen6 halamanChapter 3: Cell Structures and Their FunctionsRayumaaaBelum ada peringkat
- 7 Transport-Mechanism2Dokumen62 halaman7 Transport-Mechanism2aldrin braganzaBelum ada peringkat
- 4-Biological Membrane and Transport 21-22Dokumen21 halaman4-Biological Membrane and Transport 21-22sarahwassel2015Belum ada peringkat
- 3 PharmacokineticsDokumen36 halaman3 PharmacokineticsTanvir FahimBelum ada peringkat
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDokumen51 halamanToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieBelum ada peringkat
- Pharmacokinetics: Bahaa EL MerhabiDokumen9 halamanPharmacokinetics: Bahaa EL Merhabibahaa el merhabiBelum ada peringkat
- PharmacokineticsDokumen17 halamanPharmacokineticsღ آلَعٌرآقُيِة نِوٌر ღBelum ada peringkat
- Xenobiotics and Its Metabolism: Group 7Dokumen31 halamanXenobiotics and Its Metabolism: Group 7markganir08Belum ada peringkat
- Drug Absorption 01Dokumen15 halamanDrug Absorption 01Jannaatul Ferdous MimBelum ada peringkat
- Basic Principles General PharmacologyDokumen47 halamanBasic Principles General Pharmacologysapiah raman100% (2)
- BP604T Lecturer's Slides - CompressedDokumen119 halamanBP604T Lecturer's Slides - CompressedGyampoh SolomonBelum ada peringkat
- Drug TransportDokumen27 halamanDrug TransportYashasv BhatnagarBelum ada peringkat
- Folk Songs and Dances of SikkimDokumen5 halamanFolk Songs and Dances of SikkimShivam RaiBelum ada peringkat
- Numerical TaxonomyDokumen4 halamanNumerical TaxonomyShivam Rai100% (5)
- XL - P Chemistry (Compulsory For All XL Candidates)Dokumen2 halamanXL - P Chemistry (Compulsory For All XL Candidates)Shivam RaiBelum ada peringkat
- Cutoff Result of Third Round of B.Ed Programme For The Academic Session 2020-21Dokumen4 halamanCutoff Result of Third Round of B.Ed Programme For The Academic Session 2020-21Shivam RaiBelum ada peringkat
- XL - T ZoologyDokumen1 halamanXL - T ZoologyShivam RaiBelum ada peringkat
- NDT VTL-3-3Dokumen2 halamanNDT VTL-3-3Priyesh MauryaBelum ada peringkat
- Spice-Simulation Using LTspice Part 1Dokumen76 halamanSpice-Simulation Using LTspice Part 1suzsoltBelum ada peringkat
- Inorganic Chemistry - Lab Report 5Dokumen7 halamanInorganic Chemistry - Lab Report 5AlpBelum ada peringkat
- Understanding The Use of Ofdm in Ieee 802.16 (Wimax) : Roberto SacchiDokumen8 halamanUnderstanding The Use of Ofdm in Ieee 802.16 (Wimax) : Roberto SacchiHarald KerresBelum ada peringkat
- 351 DatasheetDokumen14 halaman351 DatasheetRafael NavarroBelum ada peringkat
- WDH-SL3 Iom M01M40N13-07 - 1542713324932Dokumen72 halamanWDH-SL3 Iom M01M40N13-07 - 1542713324932irwantino susilo100% (1)
- 4 Activity Guide and Evaluation Rubric - Unit 2 - Task 4 - Lets Talk and Share - Speaking Task - En.esDokumen8 halaman4 Activity Guide and Evaluation Rubric - Unit 2 - Task 4 - Lets Talk and Share - Speaking Task - En.esFabiana Cataño gomezBelum ada peringkat
- Evaluating Capital ProjectsDokumen254 halamanEvaluating Capital Projectsariff_sodriBelum ada peringkat
- Diagnosis and Testing: Four Wheel Drive (4WD) Systems - Electronic ShiftDokumen38 halamanDiagnosis and Testing: Four Wheel Drive (4WD) Systems - Electronic ShiftLojan Coronel José Humberto100% (1)
- Lab 3 Pre LabDokumen3 halamanLab 3 Pre LabMina VoBelum ada peringkat
- Arthashastra: Citation NeededDokumen4 halamanArthashastra: Citation NeededtusharBelum ada peringkat
- Penn State University Press Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To Philosophy & RhetoricDokumen16 halamanPenn State University Press Is Collaborating With JSTOR To Digitize, Preserve and Extend Access To Philosophy & RhetoricvanduongBelum ada peringkat
- Dell XPS 17 Quanta GM7 Rev D SchematicsDokumen39 halamanDell XPS 17 Quanta GM7 Rev D SchematicsvcompumatikBelum ada peringkat
- Automatic Fruit Image Recognition System Based On Shape and Color FeaturesDokumen2 halamanAutomatic Fruit Image Recognition System Based On Shape and Color FeaturesakshayBelum ada peringkat
- Studi Dampak Lalu Lintas Pembangunan Gudang Dan Kantor Pt. Wismilak Group Di Jalan Raya Solo SragenDokumen8 halamanStudi Dampak Lalu Lintas Pembangunan Gudang Dan Kantor Pt. Wismilak Group Di Jalan Raya Solo SragenIlung MarpaungBelum ada peringkat
- E Rich Burn Control System: With Stablesense™ TechnologyDokumen4 halamanE Rich Burn Control System: With Stablesense™ TechnologyYasir JamilBelum ada peringkat
- SOPRANO TIM SMTP Interface Developers GuideDokumen43 halamanSOPRANO TIM SMTP Interface Developers GuidenettellectBelum ada peringkat
- VI. HelicoptersDokumen147 halamanVI. HelicopterssreekanthBelum ada peringkat
- USN 18CS654: B. E. Degree (Autonomous) Sixth Semester End Examination (SEE)Dokumen2 halamanUSN 18CS654: B. E. Degree (Autonomous) Sixth Semester End Examination (SEE)Sarmi HarshaBelum ada peringkat
- Calculation Sheet Boiler Control BuildingDokumen35 halamanCalculation Sheet Boiler Control BuildingKhamal Rachmanda AdamBelum ada peringkat
- X2IPI ManualDokumen51 halamanX2IPI ManualFadiliAhmedBelum ada peringkat
- Some Observations On The Diophantine Equation Y2xa and Related ResultsDokumen12 halamanSome Observations On The Diophantine Equation Y2xa and Related ResultsJose Roberto DuarteBelum ada peringkat
- Tutorial - How To Use The Poser Format ExporterDokumen7 halamanTutorial - How To Use The Poser Format ExporterMimhypopbummilha SwuBelum ada peringkat
- Review For Final ExamDokumen29 halamanReview For Final ExamhaddanBelum ada peringkat
- Condensation and BoilingDokumen14 halamanCondensation and BoilingCrislyn Akilit Bayawa100% (1)