Anda mungkin juga menyukai
- Chronic Obstructive Pulmonary DiseaseDokumen33 halamanChronic Obstructive Pulmonary DiseasealexpharmBelum ada peringkat
- ZENICADokumen72 halamanZENICAVedadBelum ada peringkat
- Geriatrics Trauma Power Point Presentation Dr. BarbaDokumen23 halamanGeriatrics Trauma Power Point Presentation Dr. BarbagiscaamiliaBelum ada peringkat
- 1 ParkinsonsDokumen58 halaman1 ParkinsonsgautambobBelum ada peringkat
- Small Pox (CHN)Dokumen13 halamanSmall Pox (CHN)Getom NgukirBelum ada peringkat
- Cvs PracticalDokumen63 halamanCvs PracticalSreedeep TejaBelum ada peringkat
- Cerebrovascular AccidentDokumen31 halamanCerebrovascular AccidentRam ReddyBelum ada peringkat
- COPD Assessment and ManagementDokumen161 halamanCOPD Assessment and ManagementClarisse Nicole TanBelum ada peringkat
- Small PoxDokumen8 halamanSmall PoxDiazBelum ada peringkat
- Hepatitis Viruses ÍõÅà ÕDokumen85 halamanHepatitis Viruses ÍõÅà Õrasool ghaffariBelum ada peringkat
- Taufan Arif, S.Kep., NS., M.KepDokumen85 halamanTaufan Arif, S.Kep., NS., M.KepputriBelum ada peringkat
- Smallpox A Dead Disease: Dr.T.V.Rao MDDokumen46 halamanSmallpox A Dead Disease: Dr.T.V.Rao MDshravaniBelum ada peringkat
- AnemiaDokumen42 halamanAnemiameutia wardhanie ganieBelum ada peringkat
- Hematological Disorders in Geriatric PatientsDokumen18 halamanHematological Disorders in Geriatric PatientsAndre HawkBelum ada peringkat
- Cerebrovascular Accident (CVA)Dokumen71 halamanCerebrovascular Accident (CVA)nur muizzah afifah hussinBelum ada peringkat
- Geriatric 602 Final Exam Review: Osteoporosis, Pharmacology, Falls, Heat IllnessesDokumen5 halamanGeriatric 602 Final Exam Review: Osteoporosis, Pharmacology, Falls, Heat IllnessesLhen-Vincelyn LeysonBelum ada peringkat
- 2021 CVD Prevention GlsDokumen147 halaman2021 CVD Prevention GlsRuslan RidcodubskiiBelum ada peringkat
- Chronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDokumen42 halamanChronic Myeloproliferative Disorders: Matthew G. Yap, MD, FPCP, FPSHBT, FpsmoDon RaulBelum ada peringkat
- By: DR Eyad Talal: Moderator: DR I - QudaisatDokumen55 halamanBy: DR Eyad Talal: Moderator: DR I - QudaisatEyad AbdeljawadBelum ada peringkat
- An Overview Of: Acute Kidney Injury (Aki: Hasan BasriDokumen22 halamanAn Overview Of: Acute Kidney Injury (Aki: Hasan BasriDz PutraBelum ada peringkat
- PATHO Glomerular and Tubulointerstitial DiseaseDokumen43 halamanPATHO Glomerular and Tubulointerstitial DiseaseHananya ManroeBelum ada peringkat
- Degenerative Joint DiseaseDokumen35 halamanDegenerative Joint DiseaseWendy EscalanteBelum ada peringkat
- Diabetes MellitusDokumen79 halamanDiabetes Mellituskhalid saifur rahman khanBelum ada peringkat
- HRSDokumen63 halamanHRSPriya KalariaBelum ada peringkat
- Preventive CardiologyDokumen28 halamanPreventive CardiologyerizonBelum ada peringkat
- Presentasi CKDDokumen21 halamanPresentasi CKDNubli LohBelum ada peringkat
- NEJM Treatment of Patients With Cirrohsis Aug 2016Dokumen11 halamanNEJM Treatment of Patients With Cirrohsis Aug 2016risewfBelum ada peringkat
- Hypertension LecturesDokumen65 halamanHypertension LecturesAdebisiBelum ada peringkat
- Alawlaqi - Obesity FinalDokumen26 halamanAlawlaqi - Obesity FinalMotea Alawlaqi100% (1)
- Understanding Thalassemia: Causes, Symptoms and TreatmentDokumen19 halamanUnderstanding Thalassemia: Causes, Symptoms and TreatmentJayricDepalobosBelum ada peringkat
- Goodpasture Syndrome: Lung and Kidney Autoimmune DiseaseDokumen6 halamanGoodpasture Syndrome: Lung and Kidney Autoimmune DiseaseAman singhBelum ada peringkat
- Pratley New Treatments For Type 2 DiabetesDokumen85 halamanPratley New Treatments For Type 2 DiabetesMia DangaBelum ada peringkat
- AnaemiaDokumen73 halamanAnaemiamedicoprakashBelum ada peringkat
- Lecture 6 Sickle Cell AnaemiaDokumen33 halamanLecture 6 Sickle Cell AnaemiaKingsley AdebayoBelum ada peringkat
- Comprehensive: Geriatric AssessmentDokumen38 halamanComprehensive: Geriatric AssessmentDingsBelum ada peringkat
- Idiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingDokumen4 halamanIdiopathic Pulmonary Fibrosis: Optimizing The Diagnosis and Multi-Disciplinary Decision MakingAnna LiachenkoBelum ada peringkat
- HIV-associated Nephropathy (HIVAN) - UpToDate PDFDokumen22 halamanHIV-associated Nephropathy (HIVAN) - UpToDate PDFMuh Deriyatmiko BastamanBelum ada peringkat
- Urinary Stones DiseaseDokumen40 halamanUrinary Stones DiseaseRenaldy ThiorisBelum ada peringkat
- #9 Ie 8 PDFDokumen8 halaman#9 Ie 8 PDFOmar BasimBelum ada peringkat
- S0850alug 1670953860959-SEU HDokumen56 halamanS0850alug 1670953860959-SEU HAziz KhwajaBelum ada peringkat
- Wilson S DiseaseDokumen28 halamanWilson S DiseasemichaelcylBelum ada peringkat
- Peripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dokumen46 halamanPeripheral Artery Occlusive Disease: What To Do About Intermittent Claudication??Dzariyat_Azhar_9277100% (1)
- Anemia: Dr. Saranya VinothDokumen45 halamanAnemia: Dr. Saranya Vinothareeb khanBelum ada peringkat
- Emergency Department Evaluation Back PainDokumen29 halamanEmergency Department Evaluation Back PainRodolfo GorveñaBelum ada peringkat
- Anemia of Chronic Disorders (ACD)Dokumen14 halamanAnemia of Chronic Disorders (ACD)Muhamad SyaifulBelum ada peringkat
- DR Aida Lombok 3 Mei 2017 - HisfarsiDokumen39 halamanDR Aida Lombok 3 Mei 2017 - HisfarsiBasri BaslamBelum ada peringkat
- Anemia - PPT PresentationDokumen23 halamanAnemia - PPT PresentationRommel Montero RicioBelum ada peringkat
- Valvular Heart DiseaseDokumen25 halamanValvular Heart DiseaseRyan VachaparampilBelum ada peringkat
- Cerebrovascular AccidentDokumen12 halamanCerebrovascular AccidentMarvie JOiz AnteBelum ada peringkat
- Acute Coronary Syndrome Management GuidelinesDokumen56 halamanAcute Coronary Syndrome Management GuidelinesprincezastaridaBelum ada peringkat
- AnemiaDokumen71 halamanAnemiaAnsu MaliyakalBelum ada peringkat
- PericarditisDokumen29 halamanPericarditisPavin KumarBelum ada peringkat
- ALCOHOLIC LIVER DISEASEDokumen10 halamanALCOHOLIC LIVER DISEASENishanth ReddyBelum ada peringkat
- SICKLE CELL DISEASE: A CASE OF VASO-OCCLUSIVE CRISISDokumen44 halamanSICKLE CELL DISEASE: A CASE OF VASO-OCCLUSIVE CRISISNICHOLAS KAUMBA100% (1)
- Ch-13 Drugs Used in Heart FailureDokumen49 halamanCh-13 Drugs Used in Heart FailureShabrin SadikhBelum ada peringkat
- Leukaemia and Lymphoma Whats The DifferenceDokumen7 halamanLeukaemia and Lymphoma Whats The Differencepaul_calburean7899Belum ada peringkat
- 14 DyslipidemiaDokumen45 halaman14 DyslipidemiaSaniBelum ada peringkat
- Beta BlockersDokumen70 halamanBeta BlockersIrina Cabac-PogoreviciBelum ada peringkat
- Hypertensive Heart DiseaseDokumen33 halamanHypertensive Heart Diseaserini_adriani6817Belum ada peringkat
- Gastrointestinal Diseases and Disorders Sourcebook, Fifth EditionDari EverandGastrointestinal Diseases and Disorders Sourcebook, Fifth EditionBelum ada peringkat
- What Happens To Our Body After Drinking CocaDokumen3 halamanWhat Happens To Our Body After Drinking CocaPriyanka MhBelum ada peringkat
- Heart Touching ShayarisjnDokumen12 halamanHeart Touching ShayarisjnPriyanka Mh100% (1)
- History of Public Health-2Dokumen15 halamanHistory of Public Health-2Supriya VarmaBelum ada peringkat
- History of Public Health-2Dokumen15 halamanHistory of Public Health-2supriyavarmaBelum ada peringkat
- P HDokumen20 halamanP HPriyanka MhBelum ada peringkat
- Cellular Structure & FunctionDokumen57 halamanCellular Structure & FunctionPriyanka MhBelum ada peringkat
- 1 Blood: Composition of Blood (Viva)Dokumen21 halaman1 Blood: Composition of Blood (Viva)Priyanka MhBelum ada peringkat
- 1 Blood: Composition of Blood (Viva)Dokumen21 halaman1 Blood: Composition of Blood (Viva)Priyanka MhBelum ada peringkat
- Nitrifying Moving Bed Biofilm Reactor (MBBR) Biofilm and Biomass Response To Long Term Exposure To 1 CDokumen10 halamanNitrifying Moving Bed Biofilm Reactor (MBBR) Biofilm and Biomass Response To Long Term Exposure To 1 CSyamsul Bahry HarahapBelum ada peringkat
- Week8-Deception Detection (Methods)Dokumen4 halamanWeek8-Deception Detection (Methods)Sahmin SaalBelum ada peringkat
- OkinagaDokumen8 halamanOkinagaMOULIANNA8949Belum ada peringkat
- 3rd BSC Endocrinology NotesDokumen25 halaman3rd BSC Endocrinology NotesPratyashaBelum ada peringkat
- Diaphragmatic HerniaDokumen8 halamanDiaphragmatic HerniaAnonymous 9xHTwHYBelum ada peringkat
- Passion and Deceit Part VI PDFDokumen20 halamanPassion and Deceit Part VI PDFno2meBelum ada peringkat
- Pinoy Jokes!: Pupils!Dokumen4 halamanPinoy Jokes!: Pupils!joserizal666Belum ada peringkat
- Kimia Kofaktor Dan KoenzimDokumen35 halamanKimia Kofaktor Dan KoenzimSuwahono, M.PdBelum ada peringkat
- RH Isoimmunization (PritDokumen23 halamanRH Isoimmunization (PritmaezuBelum ada peringkat
- Enzymes: M. Zaharna Clin. Chem. 2009Dokumen32 halamanEnzymes: M. Zaharna Clin. Chem. 2009Ahmed GaberBelum ada peringkat
- Location and External Anatomy of The KidneysDokumen15 halamanLocation and External Anatomy of The KidneysKyla Malapit GarvidaBelum ada peringkat
- Physioex Exercise 2 Activity 5Dokumen5 halamanPhysioex Exercise 2 Activity 5Hanifa NabilaBelum ada peringkat
- Angliski Kniga VezbiDokumen6 halamanAngliski Kniga VezbiMartina JovevskaBelum ada peringkat
- Full Lab ReportDokumen5 halamanFull Lab ReportchampmorganBelum ada peringkat
- NSTSE Class 3 Answer Key Updated Paper Code 449Dokumen3 halamanNSTSE Class 3 Answer Key Updated Paper Code 449G KumarBelum ada peringkat
- Shanks 1996Dokumen5 halamanShanks 1996Sarly FebrianaBelum ada peringkat
- The Pathology of DiphtheriaDokumen5 halamanThe Pathology of DiphtheriaKamila ArifaBelum ada peringkat
- Laporan Kasus Aiman KamilaDokumen16 halamanLaporan Kasus Aiman KamilazzooooeeeeeeBelum ada peringkat
- Chronic Renal Failure Case StudyDokumen29 halamanChronic Renal Failure Case StudyMary Shine GonidaBelum ada peringkat
- VPB 111Dokumen3 halamanVPB 111Dr-Ashok KeerBelum ada peringkat
- Amer MakramDokumen16 halamanAmer MakramDRHAMADA ELWANBelum ada peringkat
- Care of Patients With Mechanical VentilatorDokumen4 halamanCare of Patients With Mechanical VentilatorIman Bee Sanayon0% (1)
- Sex and Death Chapter 2Dokumen19 halamanSex and Death Chapter 2arffurBelum ada peringkat
- Pathophysiology of PainDokumen31 halamanPathophysiology of PainJonniwal Sanusi100% (4)
- THYMUS PPT Final 7marDokumen15 halamanTHYMUS PPT Final 7marRajesh UgalmugleBelum ada peringkat
- OPP 3 Study Guide Exam 3Dokumen158 halamanOPP 3 Study Guide Exam 3Fazal DalalBelum ada peringkat
- Acute Purulent Diseases of Fingers and HandDokumen23 halamanAcute Purulent Diseases of Fingers and Handluckyswiss7776848Belum ada peringkat
- Improving RPD Retention with RPI SystemDokumen17 halamanImproving RPD Retention with RPI Systemishtiii100% (2)
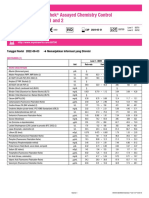
- Lyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiDokumen2 halamanLyphochek Assayed Chemistry Control Levels 1 and 2: Tanggal Revisi 2022-06-03 Menunjukkan Informasi Yang DirevisiFahmiBelum ada peringkat
- Sistem Syaraf Manusia: Nanda Fadhilah Witris Salamy, DRDokumen15 halamanSistem Syaraf Manusia: Nanda Fadhilah Witris Salamy, DRwitrisalamyBelum ada peringkat