Anda mungkin juga menyukai
- Dislipidemii Vlad 2011Dokumen40 halamanDislipidemii Vlad 2011DanielaBelum ada peringkat
- Pulmonary ThromboembolismDokumen25 halamanPulmonary ThromboembolismDanielaBelum ada peringkat
- Early Diagnosis of NeoplasisDokumen25 halamanEarly Diagnosis of NeoplasisDanielaBelum ada peringkat
- 2007 Engleza Heart FailureDokumen38 halaman2007 Engleza Heart FailureDanielaBelum ada peringkat
- Tromboza VenoasaDokumen4 halamanTromboza VenoasaDanielaBelum ada peringkat
- 12 AnaemiasDokumen52 halaman12 AnaemiasDanielaBelum ada peringkat
- 12 Hemorrhagic SyndromesDokumen16 halaman12 Hemorrhagic SyndromesDanielaBelum ada peringkat
- 11 Gastrointestinal DiseasesDokumen32 halaman11 Gastrointestinal DiseasesDanielaBelum ada peringkat
- 09 Acute Med AbdDokumen42 halaman09 Acute Med AbdDanielaBelum ada peringkat
- 07 The Valvular PatientDokumen83 halaman07 The Valvular PatientDanielaBelum ada peringkat
- 10 Patient With Liver DiseaseDokumen40 halaman10 Patient With Liver DiseaseDanielaBelum ada peringkat
- 04 Patient With HypertensionDokumen47 halaman04 Patient With HypertensionDanielaBelum ada peringkat
- 05 Patient With Acute Thoracic PainDokumen69 halaman05 Patient With Acute Thoracic PainDanielaBelum ada peringkat
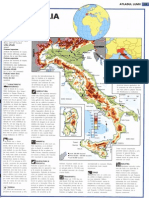
- It Ali ADokumen1 halamanIt Ali ADanielaBelum ada peringkat
- Argent in ADokumen1 halamanArgent in ADanielaBelum ada peringkat
- The Patient With Fever: Assoc. Prof. Simona DraganDokumen29 halamanThe Patient With Fever: Assoc. Prof. Simona DraganDanielaBelum ada peringkat
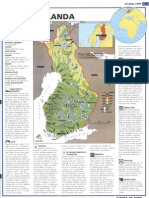
- Finland ADokumen1 halamanFinland AmamaluiraresBelum ada peringkat
- BraziliaDokumen1 halamanBraziliamamaluiraresBelum ada peringkat
- HTAcursDokumen44 halamanHTAcursDanielaBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- ETR Series: A Full Spectrum of Products To Solve Your Application NeedsDokumen106 halamanETR Series: A Full Spectrum of Products To Solve Your Application Needs周小安Belum ada peringkat
- Critical Analysis of W.H Auden Poems The PDFDokumen8 halamanCritical Analysis of W.H Auden Poems The PDFMöĤämmĔd äĹ-ŚäÁdï100% (1)
- Eco JetDokumen15 halamanEco JetJustin CoyBelum ada peringkat
- MMW ReviewerDokumen3 halamanMMW ReviewerMarcSaloj NeryBelum ada peringkat
- The Process: by Andy ZoppeltDokumen4 halamanThe Process: by Andy ZoppeltMark Stephen HuBertBelum ada peringkat
- Case AnalysisDokumen2 halamanCase AnalysisJessa San PedroBelum ada peringkat
- Crma Unit 1 Crma RolesDokumen34 halamanCrma Unit 1 Crma Rolesumop3plsdn0% (1)
- Water Filling MachineDokumen15 halamanWater Filling Machinepallab D RozarioBelum ada peringkat
- Yoga SadhguruDokumen6 halamanYoga Sadhgurucosti.sorescuBelum ada peringkat
- Sample Appellant BriefDokumen6 halamanSample Appellant BriefKaye Pascual89% (9)
- Ap, Lrrsisal of Roentgenograph, Ic: I SsayDokumen30 halamanAp, Lrrsisal of Roentgenograph, Ic: I SsayMindaugasStacevičiusBelum ada peringkat
- Liftchain (LC2A) Catalog AirHoistDokumen10 halamanLiftchain (LC2A) Catalog AirHoisteduardshark100% (1)
- Essential Calculus Skills Practice Workbook With Full SolutionsDokumen528 halamanEssential Calculus Skills Practice Workbook With Full SolutionsGerardo Navarro Sánchez94% (65)
- Regression Analysis Random Motors ProjectDokumen22 halamanRegression Analysis Random Motors ProjectPrateek AgrawalBelum ada peringkat
- Resume: Satyam KumarDokumen3 halamanResume: Satyam KumarEr Satyam Kumar KrantiBelum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar PustakaMel DaBelum ada peringkat
- Iodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04Dokumen12 halamanIodide and Bromide Ions in Brackish Water, Seawater, and Brines D 3869 - 04stevgonBelum ada peringkat
- 15 Benefits of CyclingDokumen8 halaman15 Benefits of CyclingJoycs PintoBelum ada peringkat
- Tips For A Healthy PregnancyDokumen2 halamanTips For A Healthy PregnancyLizaBelum ada peringkat
- Dharmakirti39s Commentary On ChakrasamvaraDokumen15 halamanDharmakirti39s Commentary On ChakrasamvaraThiago AlbuquerqueBelum ada peringkat
- Science Magazine February 2020Dokumen133 halamanScience Magazine February 2020Elena González GonzálezBelum ada peringkat
- Clinical Biomechanics: Leigh W. Marshall, Stuart M. McgillDokumen4 halamanClinical Biomechanics: Leigh W. Marshall, Stuart M. McgillMichael JunBelum ada peringkat
- Chapter 7 - Stress - TransformationsDokumen21 halamanChapter 7 - Stress - TransformationsroselleBelum ada peringkat
- Raneem AlbazazDokumen33 halamanRaneem AlbazazGordana PuzovicBelum ada peringkat
- 2nd APJ Abdul Kalam Essay Writing CompetitionDokumen2 halaman2nd APJ Abdul Kalam Essay Writing CompetitionANURAG SINGHBelum ada peringkat
- Usp Description and SolubilityDokumen1 halamanUsp Description and SolubilityvafaashkBelum ada peringkat
- Model Detailed Project Report: Animal Feed Making UnitDokumen19 halamanModel Detailed Project Report: Animal Feed Making UnitShashi ShekharBelum ada peringkat
- Keyword 4: Keyword: Strength of The Mixture of AsphaltDokumen2 halamanKeyword 4: Keyword: Strength of The Mixture of AsphaltJohn Michael GeneralBelum ada peringkat
- CCNA Training New CCNA - RSTPDokumen7 halamanCCNA Training New CCNA - RSTPokotete evidenceBelum ada peringkat
- ACR39U-U1: (USB Type A) Smart Card ReaderDokumen8 halamanACR39U-U1: (USB Type A) Smart Card Readersuraj18in4uBelum ada peringkat