Anda mungkin juga menyukai
- Guide to Antipsychotics for SchizophreniaDokumen24 halamanGuide to Antipsychotics for SchizophreniaKhadija ArshadBelum ada peringkat
- Psychotherapeutic Drugs GuideDokumen12 halamanPsychotherapeutic Drugs Guidecamile buhanginBelum ada peringkat
- Overview of Psychotropic DrugsDokumen7 halamanOverview of Psychotropic Drugsnad101Belum ada peringkat
- Psychotropic Drugs: Bryan Mae H. DegorioDokumen65 halamanPsychotropic Drugs: Bryan Mae H. DegorioBryan Mae H. Degorio100% (2)
- Obat-Obat Psychiatry - 1 2018Dokumen104 halamanObat-Obat Psychiatry - 1 2018Christo LimbongBelum ada peringkat
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDokumen29 halamanPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaBelum ada peringkat
- Antidepressant Therapy AlgorithmDokumen12 halamanAntidepressant Therapy AlgorithmZubair Mahmood KamalBelum ada peringkat
- Neurobiology of Depression: Guide-Dr. Vijay Niranjan SirDokumen42 halamanNeurobiology of Depression: Guide-Dr. Vijay Niranjan SirPriyash JainBelum ada peringkat
- 1: Adhd: Scientific Name Dose CommentsDokumen4 halaman1: Adhd: Scientific Name Dose CommentsSadiq Abdo92Belum ada peringkat
- Introduction To NeuropharmacologyDokumen6 halamanIntroduction To Neuropharmacologyammarhafez78100% (1)
- Presented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Dokumen17 halamanPresented By:-11081506 (Ridhi) 11081524 (Khushboo) 11081560 (Shiny) 11081542 (Sakshi)Akanksha KapoorBelum ada peringkat
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDokumen8 halamanCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniBelum ada peringkat
- Brain Imaging in PsychiatryDokumen7 halamanBrain Imaging in PsychiatryKaram Ali ShahBelum ada peringkat
- Current Clinical Strategies: Handbook of Psychiatric DrugsDokumen72 halamanCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116Belum ada peringkat
- Antidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsDokumen3 halamanAntidepressants Comparison Guide Most Commonly Prescribed: Recommend GenericsCarina ColtuneacBelum ada peringkat
- Dosage and Pharmacology of Antipsychotics - UpToDate ...Dokumen4 halamanDosage and Pharmacology of Antipsychotics - UpToDate ...Dragutin PetrićBelum ada peringkat
- Biological Aspects of OCD SeminarDokumen60 halamanBiological Aspects of OCD Seminarneha mattikoppaBelum ada peringkat
- AripripazoleDokumen13 halamanAripripazoleOneng IfayaniBelum ada peringkat
- Antipsychotic DrugsDokumen54 halamanAntipsychotic DrugsJackBelum ada peringkat
- Pharmacology and Toxicology of Antidepressants and AntipsychoticsDokumen50 halamanPharmacology and Toxicology of Antidepressants and AntipsychoticsPintu Bhushan MitraBelum ada peringkat
- TrOn ReferencesDokumen11 halamanTrOn ReferencesAnonymous CbnCgjBelum ada peringkat
- Geriatric Giants - DR SeymourDokumen108 halamanGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Bms166 Slide Antipsychotic AntidepressantDokumen52 halamanBms166 Slide Antipsychotic AntidepressantErmanto D'PhytoxzBelum ada peringkat
- Introduction to Pharmacology I (Lecture 1Dokumen75 halamanIntroduction to Pharmacology I (Lecture 1Basil Elbushra Ahmed DomiBelum ada peringkat
- B /G C U I R: Anti-PsychoticsDokumen2 halamanB /G C U I R: Anti-PsychoticsErsy Sakti ilhamBelum ada peringkat
- Pediatrics: St. Elizabeth Family Medicine Residency ProgramDokumen9 halamanPediatrics: St. Elizabeth Family Medicine Residency Programwingchun108tekBelum ada peringkat
- CNS StimulantDokumen26 halamanCNS StimulantIslam Abdo50% (2)
- Anxiety and Psychosexual Disorders in ChildDokumen60 halamanAnxiety and Psychosexual Disorders in ChildAnnalesa BarkerBelum ada peringkat
- Hess BenoitWritingHistoryPsychiatryDokumen8 halamanHess BenoitWritingHistoryPsychiatryIvo VarlaBelum ada peringkat
- PHARMACOLOGY OF PSYCHOSIS AND MANIADokumen53 halamanPHARMACOLOGY OF PSYCHOSIS AND MANIAlavanyakakarlaBelum ada peringkat
- Adult Psychiatry I: Paper B Syllabic Content 7.1Dokumen69 halamanAdult Psychiatry I: Paper B Syllabic Content 7.1JasonBelum ada peringkat
- AntidepressantsDokumen59 halamanAntidepressantsanon_189054600100% (2)
- S-GA Use in Pregnancy Linked to Increased RisksDokumen9 halamanS-GA Use in Pregnancy Linked to Increased RisksDian Oktaria SafitriBelum ada peringkat
- Neuroleptic Advers ReactionDokumen65 halamanNeuroleptic Advers Reactionayu yulianti100% (1)
- Case Study 142: Assessing Suicide Risk in a Depressed Elderly PatientDokumen5 halamanCase Study 142: Assessing Suicide Risk in a Depressed Elderly PatientPatricia Ann Nicole ReyesBelum ada peringkat
- Treatment Resistant OCD .Dokumen55 halamanTreatment Resistant OCD .Dr viren SolankiBelum ada peringkat
- RECEPTORS, TRANSPORTERS, ENZYMES & ION CHANNELSDokumen58 halamanRECEPTORS, TRANSPORTERS, ENZYMES & ION CHANNELSDeepu Vijay100% (1)
- Terms in The Field of PsychiatryDokumen18 halamanTerms in The Field of PsychiatryOchie YecyecanBelum ada peringkat
- Esketamine For Treatment Resistant DepressionDokumen13 halamanEsketamine For Treatment Resistant DepressionJuan ParedesBelum ada peringkat
- PsychopharmacologyDokumen50 halamanPsychopharmacologyapi-3703352Belum ada peringkat
- Tranylcypromine in Mind Part I - Review of P - 2017 - European Neuropsychopharm PDFDokumen17 halamanTranylcypromine in Mind Part I - Review of P - 2017 - European Neuropsychopharm PDFdanilomarandolaBelum ada peringkat
- Third Generation Antipsychotic DrugsDokumen45 halamanThird Generation Antipsychotic DrugsGabriela Drima100% (1)
- 01 Introduction To PsychiatryDokumen29 halaman01 Introduction To PsychiatryPatricia Denise OrquiaBelum ada peringkat
- Tranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFDokumen18 halamanTranylcypromine in Mind Part II - Review of Clinical PH - 2017 - European Neuro PDFdanilomarandolaBelum ada peringkat
- INTRODUCTION TO NEUROPHARMACOLOGYyyDokumen27 halamanINTRODUCTION TO NEUROPHARMACOLOGYyyEbad RazviBelum ada peringkat
- Role of homoeopathy in psychological disordersDokumen6 halamanRole of homoeopathy in psychological disordersMadhu Ronda100% (1)
- MC IIIA Topics: Midterm Material. Won't Be in The Final Exam, Only Antiparkinsonian IncludedDokumen138 halamanMC IIIA Topics: Midterm Material. Won't Be in The Final Exam, Only Antiparkinsonian IncludedToqa ElmansouryBelum ada peringkat
- Dr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityDokumen41 halamanDr. Jagan Associate Professor of Pharmacology HOD - para Clinical Department Texila American UniversityredderdatBelum ada peringkat
- Methods Used in EpidemologyDokumen53 halamanMethods Used in EpidemologySameera banuBelum ada peringkat
- Substance Abuse Power PointDokumen65 halamanSubstance Abuse Power PointFletcher1980Belum ada peringkat
- B2B Psychopharmacology 2015Dokumen128 halamanB2B Psychopharmacology 2015Soleil DaddouBelum ada peringkat
- A List A Statistical Definition For The CICM Fellowship ExamDokumen5 halamanA List A Statistical Definition For The CICM Fellowship ExamSimon WongBelum ada peringkat
- Medicines in PregnancyDokumen18 halamanMedicines in Pregnancymominur11Belum ada peringkat
- Depression Medications ExplainedDokumen5 halamanDepression Medications ExplainedxyzBelum ada peringkat
- Psychopharma 1Dokumen7 halamanPsychopharma 1Mitchee Zialcita100% (1)
- Intro Child PsychiatryDokumen122 halamanIntro Child PsychiatryayunisallehBelum ada peringkat
- Antidepressants AntidepressantsDokumen38 halamanAntidepressants AntidepressantsjaneBelum ada peringkat
- Drug Treatment of PsychosisDokumen57 halamanDrug Treatment of PsychosisDaniel WangBelum ada peringkat
- Psychopharmacology in PsychiatryDokumen94 halamanPsychopharmacology in PsychiatryOslo SaputraBelum ada peringkat
- Drug Use and Abuse Canadian 1st Edition Maisto Test BankDokumen12 halamanDrug Use and Abuse Canadian 1st Edition Maisto Test Bankkarenyoungsbpmkaxioz100% (16)
- The Five Illicit DrugsDokumen7 halamanThe Five Illicit DrugsAlethiaBelum ada peringkat
- Drug Abuse Guide by Laxmimam - Presented by RoopaDokumen47 halamanDrug Abuse Guide by Laxmimam - Presented by Roopakrishna100% (3)
- Opioid Abusers Prefer Hydrocodone or Oxycodone For Different ReasonsDokumen1 halamanOpioid Abusers Prefer Hydrocodone or Oxycodone For Different Reasonsobx4everBelum ada peringkat
- Sat, Jun 25, 2022 062-0002719-22 0105 35001: MSP Hart Post OceanaDokumen3 halamanSat, Jun 25, 2022 062-0002719-22 0105 35001: MSP Hart Post OceanaFergus BurnsBelum ada peringkat
- Test Bank For Drugs Society and Human Behavior 17th EditionDokumen7 halamanTest Bank For Drugs Society and Human Behavior 17th EditionHarry Seldon100% (29)
- Bahasa Inggris (NARKOBA)Dokumen7 halamanBahasa Inggris (NARKOBA)jimtumangkeBelum ada peringkat
- OklahomaDokumen86 halamanOklahomaAdnan AnwarBelum ada peringkat
- Hydrocodone/Acetaminophen Tablets & Capsules: Media ImagesDokumen9 halamanHydrocodone/Acetaminophen Tablets & Capsules: Media ImagesjavasoloBelum ada peringkat
- Kicking The Habit: The Opioid Crisis and America's Addiction To ProhibitionDokumen24 halamanKicking The Habit: The Opioid Crisis and America's Addiction To ProhibitionCato InstituteBelum ada peringkat
- Katzung SummaryDokumen60 halamanKatzung Summaryedwarbc1Belum ada peringkat
- Caroline Jean Acker - Creating The American Junkie - Addiction Research in The Classic Era of Narcotic Control - The Johns Hopkins University Press (2002)Dokumen289 halamanCaroline Jean Acker - Creating The American Junkie - Addiction Research in The Classic Era of Narcotic Control - The Johns Hopkins University Press (2002)Matteo RiveraBelum ada peringkat
- Alcohol Lecture Grade 8Dokumen46 halamanAlcohol Lecture Grade 8Albert Ian CasugaBelum ada peringkat
- Cdi8 Lesson 1Dokumen8 halamanCdi8 Lesson 1juje jaulaBelum ada peringkat
- Q2 Health PPT WK 1 FundalesDokumen43 halamanQ2 Health PPT WK 1 FundalesAnne Nicole FloresBelum ada peringkat
- Drug Study For AMCDokumen3 halamanDrug Study For AMCTrixia RiveraBelum ada peringkat
- Drug Abuse PPT 20-7-18Dokumen38 halamanDrug Abuse PPT 20-7-18shashiBelum ada peringkat
- Sedative and HypnoticsDokumen26 halamanSedative and HypnoticsZarish IftikharBelum ada peringkat
- Drug Education in The PhilippinesDokumen32 halamanDrug Education in The PhilippinesTrixie Ann MenesesBelum ada peringkat
- Anti Anxiety DrugsDokumen26 halamanAnti Anxiety DrugsSANJIV KUMAR YADAV100% (1)
- Henry County Drug Operation November 2020 Media ReleaseDokumen24 halamanHenry County Drug Operation November 2020 Media ReleasePat ThomasBelum ada peringkat
- Naloxone: What Are Some Signs of An Opioid Overdose?Dokumen4 halamanNaloxone: What Are Some Signs of An Opioid Overdose?Fajriah SaraswatiBelum ada peringkat
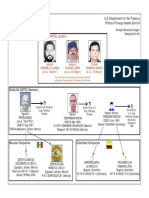
- Sinaloa Cartel Press ChartDokumen1 halamanSinaloa Cartel Press ChartcaireBelum ada peringkat
- Rekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFDokumen10 halamanRekapitulasi Laporan Narkotika: NO Nama Satuan Stok Awal Pemasukan PBFMiftah JannahBelum ada peringkat
- Drug Education: Dr. Ariel C. ManlusocDokumen213 halamanDrug Education: Dr. Ariel C. ManlusocSims LeonorBelum ada peringkat
- Crisis HotlinesDokumen1 halamanCrisis Hotlinesapi-360334932Belum ada peringkat
- Template Aging Obat Jan 24Dokumen654 halamanTemplate Aging Obat Jan 24fennyrahmaBelum ada peringkat
- AmsterdamLiquidXno1 vendor profile and product listDokumen11 halamanAmsterdamLiquidXno1 vendor profile and product listArrush AhujaBelum ada peringkat
- Eng PDFDokumen88 halamanEng PDFChoga ArlandoBelum ada peringkat
- Essay 2Dokumen6 halamanEssay 2api-550007180Belum ada peringkat