Anda mungkin juga menyukai
- Mechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingDari EverandMechanisms of Drug Toxicity: Proceedings of the Third International Pharmacological MeetingH. RaškováBelum ada peringkat
- ROA of AnimalsDokumen23 halamanROA of AnimalsMr.White sheep MusicBelum ada peringkat
- Routeadministration 4 PDFDokumen15 halamanRouteadministration 4 PDFLast StoryBelum ada peringkat
- Evaluation of Analgesic AgentsDokumen61 halamanEvaluation of Analgesic Agentsvasanth vijayBelum ada peringkat
- Mouse Handling Techniques PacketDokumen24 halamanMouse Handling Techniques PacketLovely Ann AyapanaBelum ada peringkat
- AntipyreticsDokumen5 halamanAntipyreticsClark LopezBelum ada peringkat
- Practice Pharmacology QuestionsDokumen34 halamanPractice Pharmacology QuestionsWilliam StaffBelum ada peringkat
- Diuretics Diuretics: Presentation By: DR Prabhakar Moderator: DR DamDokumen56 halamanDiuretics Diuretics: Presentation By: DR Prabhakar Moderator: DR DamPrabhakar KumarBelum ada peringkat
- Aiman - Patient Case Study ReportDokumen14 halamanAiman - Patient Case Study Reportezwan007100% (1)
- Micro Chart #3 - Italics OnlyDokumen27 halamanMicro Chart #3 - Italics Onlyapi-26938624100% (1)
- Protein Synthesis InhibitorsDokumen25 halamanProtein Synthesis InhibitorsSawsan Z. JwaiedBelum ada peringkat
- Normality N MolarityDokumen10 halamanNormality N Molaritynavigcp100% (9)
- Corticosteroids: Prof. Dr. Shah MuradDokumen51 halamanCorticosteroids: Prof. Dr. Shah MuradnehascribdjoshiBelum ada peringkat
- Challenges To Implementation of The Pharmaceutical Care Practice in Davao City.Dokumen11 halamanChallenges To Implementation of The Pharmaceutical Care Practice in Davao City.JessieLynMolinaBelum ada peringkat
- Indomethacin 392Dokumen17 halamanIndomethacin 392Mahadie Hasan JahadBelum ada peringkat
- Organisational Structure StudyDokumen49 halamanOrganisational Structure Studymiliya_abrahamBelum ada peringkat
- Indomethacin: By: Hedy Mae Bautista and Ana Francesca JacintoDokumen10 halamanIndomethacin: By: Hedy Mae Bautista and Ana Francesca JacintoAna FrancescaBelum ada peringkat
- Lab Techniques in MiceDokumen53 halamanLab Techniques in MiceSilverEva4Belum ada peringkat
- AtropineDokumen14 halamanAtropineKrazygopa BalorBelum ada peringkat
- Chapter 1 Lecture Quality ControlDokumen23 halamanChapter 1 Lecture Quality ControlJudah Israel LescanoBelum ada peringkat
- AntidotesDokumen21 halamanAntidotesSandeep MahyavanshiBelum ada peringkat
- 61 80 Otc DrugsDokumen8 halaman61 80 Otc DrugsIra YaoBelum ada peringkat
- DiureticsDokumen49 halamanDiureticsamara cheemaBelum ada peringkat
- Introduction To Pharmacoepidemiology 2015 PDFDokumen20 halamanIntroduction To Pharmacoepidemiology 2015 PDFNovria Rizki HarahapBelum ada peringkat
- Antifungal Agent PPT PresentationDokumen38 halamanAntifungal Agent PPT Presentationdinberu tadesseBelum ada peringkat
- 9autacoids 14010v9023022 Phpapp02Dokumen109 halaman9autacoids 14010v9023022 Phpapp02h3cn1r3100% (1)
- NSAIDSDokumen19 halamanNSAIDSDonna Kelly DuranBelum ada peringkat
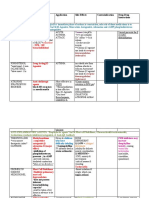
- Drug Name Mechanism Application Side Effects Contraindication Drug-Drug InteractionsDokumen3 halamanDrug Name Mechanism Application Side Effects Contraindication Drug-Drug Interactionsazhar hussinBelum ada peringkat
- Organoleptic TestingDokumen27 halamanOrganoleptic TestingmukhtarBelum ada peringkat
- Community Pharmacy Benchmarking Guideline 2011Dokumen33 halamanCommunity Pharmacy Benchmarking Guideline 2011omer tariqBelum ada peringkat
- Unit Operations in Secondary ManufacturingDokumen11 halamanUnit Operations in Secondary ManufacturingJoyce Marian BelonguelBelum ada peringkat
- Bronchodilator & Other Drugs Used in AsthmaDokumen15 halamanBronchodilator & Other Drugs Used in AsthmaGenta JagadBelum ada peringkat
- Gonadal Hormones and InhibitorsDokumen101 halamanGonadal Hormones and Inhibitors2012100% (4)
- Sulfonamides: By: Dr. Shruthi Rammohan Final Year PG Pharmacology RRMCHDokumen45 halamanSulfonamides: By: Dr. Shruthi Rammohan Final Year PG Pharmacology RRMCHAli Veer Ali VeerBelum ada peringkat
- Collection of Blood Sample From Experimental AnimalsDokumen12 halamanCollection of Blood Sample From Experimental AnimalslovehopeBelum ada peringkat
- Total Quality Management in Pharmaceuticals PDFDokumen11 halamanTotal Quality Management in Pharmaceuticals PDFNarongchai PongpanBelum ada peringkat
- 47-Drug Acting On Skin and MucousDokumen3 halaman47-Drug Acting On Skin and MucousMuhammad Sarmad MalikBelum ada peringkat
- Practical 1-Far 161-FinishDokumen10 halamanPractical 1-Far 161-FinishZulkifli Khairuddin100% (1)
- Adverse Drug ReactionDokumen24 halamanAdverse Drug ReactionGopal pokhrelBelum ada peringkat
- K46 Pharmacology of Anthelminthics, Antiprotozoal, & Antimalaria (Farmakologi)Dokumen78 halamanK46 Pharmacology of Anthelminthics, Antiprotozoal, & Antimalaria (Farmakologi)ayapillaiBelum ada peringkat
- The Role of Hospital Pharmacist As PreceptorDokumen14 halamanThe Role of Hospital Pharmacist As PreceptorKlub 'Apoteker' IndonesiaBelum ada peringkat
- Paracetamol PDFDokumen49 halamanParacetamol PDFEhb90210Belum ada peringkat
- Antibiotics: Means Against LifeDokumen13 halamanAntibiotics: Means Against Lifeshankul kumar100% (1)
- Antiretroviral Agents 2017Dokumen38 halamanAntiretroviral Agents 2017Iman SaksoukBelum ada peringkat
- 3 ConstipationDokumen18 halaman3 Constipationكسلان اكتب اسميBelum ada peringkat
- Allergic Rhinitis PDFDokumen3 halamanAllergic Rhinitis PDFdrbilalmunirBelum ada peringkat
- Exploratory Study of Self-Medication Practices Among StudentsDokumen5 halamanExploratory Study of Self-Medication Practices Among StudentsN SBelum ada peringkat
- Diuretics and Other Pharmacological ActivityDokumen8 halamanDiuretics and Other Pharmacological ActivityMohan KalaskarBelum ada peringkat
- Dr. Rathnakar U.P.: Departments of Pharmacology Kasturba Medical College, MangaloreDokumen26 halamanDr. Rathnakar U.P.: Departments of Pharmacology Kasturba Medical College, MangaloreDr.U.P.Rathnakar.MD.DIH.PGDHMBelum ada peringkat
- New Drug Development and Approval ProcessDokumen19 halamanNew Drug Development and Approval ProcessKristine Aubrey AlvarezBelum ada peringkat
- Abbreviation Meaning: AbdominalDokumen3 halamanAbbreviation Meaning: AbdominalMariel GentilesBelum ada peringkat
- AutacoidsDokumen38 halamanAutacoidsdrmayangBelum ada peringkat
- Lecture 1 PDFDokumen75 halamanLecture 1 PDFBasil Elbushra Ahmed DomiBelum ada peringkat
- Dr. Rathnakar U.P.: Department of Pharmacology Kasturba Medical College, MangaloreDokumen25 halamanDr. Rathnakar U.P.: Department of Pharmacology Kasturba Medical College, MangaloreDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Adrenocorticosteroids and Adrenocortical AntagonistsDokumen53 halamanAdrenocorticosteroids and Adrenocortical AntagonistsKetan PatelBelum ada peringkat
- ExcretionDokumen35 halamanExcretionHely PatelBelum ada peringkat
- Anthelmintic Introduction-Diethylcarbamazine CitrateDokumen2 halamanAnthelmintic Introduction-Diethylcarbamazine CitrateEric Frazad MagsinoBelum ada peringkat
- Nurse Orientation - NarcoticsDokumen25 halamanNurse Orientation - NarcoticsSalma MustafaBelum ada peringkat
- Sistem Komunikasi Antar-Sel: Nervous System Endocrine System Immune SystemDokumen38 halamanSistem Komunikasi Antar-Sel: Nervous System Endocrine System Immune SystemtangkasBelum ada peringkat
- OTC Drug ListDokumen7 halamanOTC Drug ListHong Diem100% (1)
- Price List (2 Feb'24) HEC-P0005-2024Dokumen13 halamanPrice List (2 Feb'24) HEC-P0005-2024stts motorBelum ada peringkat
- Handbook of Essential Pharmacokinetics, Pharmacodynamics, and Drug Metabolism For Industrial ScientistDokumen302 halamanHandbook of Essential Pharmacokinetics, Pharmacodynamics, and Drug Metabolism For Industrial Scientistdavid_dung100% (2)
- Question Bank BiopharmDokumen6 halamanQuestion Bank BiopharmHrushikesh JadhavBelum ada peringkat
- Bioactive Compounds in PlantsDokumen32 halamanBioactive Compounds in PlantsTilahun BelaynehBelum ada peringkat
- Sun Pharmaceutical Industries LTD.: Sun Pharma India Prescription RankingDokumen8 halamanSun Pharmaceutical Industries LTD.: Sun Pharma India Prescription RankingOmkar DandekarBelum ada peringkat
- Notice: Reports and Guidance Documents Availability, Etc.: Guidance Documents Annual ListDokumen46 halamanNotice: Reports and Guidance Documents Availability, Etc.: Guidance Documents Annual ListJustia.comBelum ada peringkat
- Laporan Obat Ed 2016: No. Nama Barang Unit ED Jumlah HPPDokumen3 halamanLaporan Obat Ed 2016: No. Nama Barang Unit ED Jumlah HPPIeie MawonBelum ada peringkat
- Merck Vitamin K Package Insert - Aquamephyton PIDokumen5 halamanMerck Vitamin K Package Insert - Aquamephyton PIDonna100% (10)
- Study GuideDokumen8 halamanStudy GuideericBelum ada peringkat
- Extra Pyramidal Symptoms AdvanceDokumen5 halamanExtra Pyramidal Symptoms AdvanceMr. Psycho Sam100% (2)
- MD Pharmacology Question Papers 2019-06-17 11.48.23 PDFDokumen8 halamanMD Pharmacology Question Papers 2019-06-17 11.48.23 PDFVijendra RBelum ada peringkat
- Guidelines For ATC Classification and DDDDokumen251 halamanGuidelines For ATC Classification and DDDJose De La Cruz De La OBelum ada peringkat
- Bromhexini Syrup LeafletDokumen2 halamanBromhexini Syrup LeafletAlbert RenardBelum ada peringkat
- 18 - Availability of Nembutal-1-10Dokumen10 halaman18 - Availability of Nembutal-1-10koko100% (2)
- MedicamenteDokumen2 halamanMedicamenteAle LiBelum ada peringkat
- Drug Study (Tapazole)Dokumen3 halamanDrug Study (Tapazole)Izza DeloriaBelum ada peringkat
- CEFUROXIMEDokumen1 halamanCEFUROXIMEAnna LaritaBelum ada peringkat
- Chemotherapy QuizDokumen5 halamanChemotherapy Quizkamie155Belum ada peringkat
- HNPDokumen10 halamanHNPPattia1980Belum ada peringkat
- SEO Template For New Content: Target Keywords: Medical DetoxDokumen20 halamanSEO Template For New Content: Target Keywords: Medical DetoxEnrique VilcaBelum ada peringkat
- List of Pharmaceutical Company in VadodaraDokumen12 halamanList of Pharmaceutical Company in Vadodarasnmv6100% (3)
- ATI Flash Cards 06, Medications Affecting The Cardiovascular SystemDokumen48 halamanATI Flash Cards 06, Medications Affecting The Cardiovascular SystemWiilka QarnigaBelum ada peringkat
- DRUGS EDUC. QuestionnaireDokumen7 halamanDRUGS EDUC. QuestionnaireDioner Ray100% (5)
- Stok Benang Kamar OperasiDokumen5 halamanStok Benang Kamar OperasirendyBelum ada peringkat
- Safe Administrations of Medications (Draft Chapter)Dokumen74 halamanSafe Administrations of Medications (Draft Chapter)Caleb FellowesBelum ada peringkat
- Difference Between Agonist and Antagonist DrugsDokumen5 halamanDifference Between Agonist and Antagonist DrugsSana Sheikh KashifBelum ada peringkat
- Rational Use of Drugs-IDokumen38 halamanRational Use of Drugs-IUmair Mazhar100% (1)
- Cns Stimulants: Convulsants - Analeptics - PsychostimulantsDokumen4 halamanCns Stimulants: Convulsants - Analeptics - Psychostimulantss.khan9211rediffmail.comBelum ada peringkat
- MyasteniaDokumen7 halamanMyastenialmcarmonaBelum ada peringkat