Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Nursing Care Plan For HypoglycemiaDokumen3 halamanNursing Care Plan For HypoglycemiaCyrus De Asis83% (53)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- (Barash) Clinical Anesthesia (6th Ed.)Dokumen3.968 halaman(Barash) Clinical Anesthesia (6th Ed.)menocide_ss67% (3)
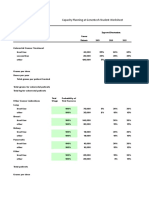
- Genentech Student Worksheet - ResultDokumen10 halamanGenentech Student Worksheet - ResultArijit MajiBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Activity Intolerance NCPDokumen7 halamanActivity Intolerance NCPMariquita BuenafeBelum ada peringkat
- In Vitro Evaluation of Aerosol Delivery - Complementaria - Semana 3Dokumen7 halamanIn Vitro Evaluation of Aerosol Delivery - Complementaria - Semana 3natalia muñozBelum ada peringkat
- NACO ART Guidelines 2013Dokumen122 halamanNACO ART Guidelines 2013RohitKumarBelum ada peringkat
- Adjustment and Impulse Control DisordersDokumen19 halamanAdjustment and Impulse Control DisordersArchana50% (4)
- Comparison of Platelet Count Methods in The Presence of Interfering Substances - Marionneaux 2010Dokumen1 halamanComparison of Platelet Count Methods in The Presence of Interfering Substances - Marionneaux 2010Steven Marionneaux, MS, MT(ASCP)Belum ada peringkat
- Positioning QuestionsDokumen5 halamanPositioning QuestionsShara SampangBelum ada peringkat
- Paediatric Lecture Guide by Obasi Chinedu-1 PDFDokumen390 halamanPaediatric Lecture Guide by Obasi Chinedu-1 PDFsamycoolqBelum ada peringkat
- Admit Card 6 SemDokumen3 halamanAdmit Card 6 SemRitik mishraBelum ada peringkat
- Clinical Practice Guidelines On Hepatitis Delta VirusDokumen28 halamanClinical Practice Guidelines On Hepatitis Delta VirusRadu IonescuBelum ada peringkat
- Activity 1Dokumen4 halamanActivity 1KyleRepolidon MoralesBelum ada peringkat
- English For Nursing Topic 13 Explaining MedicationDokumen6 halamanEnglish For Nursing Topic 13 Explaining MedicationEha Huwaida HayatiBelum ada peringkat
- SadsadDokumen3 halamanSadsadDalo ZeronBelum ada peringkat
- Assignment Submitted To DR Iqra Naz 70063678 Habiba Jameel DPT 10 Semester. Topic: ArthritisDokumen10 halamanAssignment Submitted To DR Iqra Naz 70063678 Habiba Jameel DPT 10 Semester. Topic: ArthritisMuiz SaddozaiBelum ada peringkat
- Gout Part 1 ACR-12-0014-1Dokumen16 halamanGout Part 1 ACR-12-0014-1vitauxianaBelum ada peringkat
- Annals of XII International Symposium On Vasoactive PeptidesDokumen99 halamanAnnals of XII International Symposium On Vasoactive PeptidesDaisy Motta SantosBelum ada peringkat
- Stress Ulcer Ditinjau Dari Aspek Patofisiologi Dan TreatmentDokumen16 halamanStress Ulcer Ditinjau Dari Aspek Patofisiologi Dan TreatmentJufri NstBelum ada peringkat
- Different Types of AsthmaDokumen16 halamanDifferent Types of AsthmaAmira Saidin0% (1)
- Systemic Lupus ErythematosusDokumen9 halamanSystemic Lupus ErythematosusTheeya QuigaoBelum ada peringkat
- Z Track InjectionsDokumen2 halamanZ Track InjectionssusanloveperegrinoBelum ada peringkat
- Cardiovascular System Anatomy: The HeartDokumen5 halamanCardiovascular System Anatomy: The HeartSyafiq RozaliBelum ada peringkat
- Pressure UlcersDokumen43 halamanPressure UlcersZubda Butt100% (2)
- Mindfulness-Based Cognitive Therapy For DepressionDokumen10 halamanMindfulness-Based Cognitive Therapy For DepressionCMValmaBelum ada peringkat
- Castro Et Al. ProtocoloDokumen10 halamanCastro Et Al. ProtocoloFrancisco Alfonso Burgos JuliánBelum ada peringkat
- Chapter 14 MisDokumen59 halamanChapter 14 MisKeith Mark AlmarinesBelum ada peringkat
- Bolus Vs Continuous Nasogastric Feeds in Mechanically VentilatedDokumen17 halamanBolus Vs Continuous Nasogastric Feeds in Mechanically VentilatedMirzania Mahya FathiaBelum ada peringkat
- CDC MMR, MMR+V, MMRV Seizure RatesDokumen4 halamanCDC MMR, MMR+V, MMRV Seizure RatesVaccineInformation83% (6)
- Cardiac Case Study NDDokumen11 halamanCardiac Case Study NDapi-313165458Belum ada peringkat