Anda mungkin juga menyukai
- Chapter 20 - The KidneyDokumen24 halamanChapter 20 - The KidneyAgnieszka WisniewskaBelum ada peringkat
- SN 1Dokumen9 halamanSN 1lilisBelum ada peringkat
- Glomerulonephritis: Glomerulonephritis Is Also Known As Glomerular Nephritis (GN) or Glomerular Disease. It IsDokumen3 halamanGlomerulonephritis: Glomerulonephritis Is Also Known As Glomerular Nephritis (GN) or Glomerular Disease. It Isjan_m25Belum ada peringkat
- DISC, Drugs, Infection, Thick Basal MembraneDokumen5 halamanDISC, Drugs, Infection, Thick Basal MembraneHOPEBelum ada peringkat
- Summary of Renal Disorders - 9.11.19Dokumen4 halamanSummary of Renal Disorders - 9.11.19Nicole Juliette CCBelum ada peringkat
- Glomerular Diseases My NotesDokumen5 halamanGlomerular Diseases My Notesmalar_km43Belum ada peringkat
- อ.บัญชา Glomerular - disease - handoutพี่ดาวDokumen142 halamanอ.บัญชา Glomerular - disease - handoutพี่ดาวNitaan TangsritrakulBelum ada peringkat
- Glomerulonephritis: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2019Dokumen68 halamanGlomerulonephritis: Prof DR DR Haerani Rasyid, Mkes, SPPD, KGH, SPGK Tim Ginjal Hipertensi Unhas 2019uzan100% (1)
- Acute Nephritic SyndromeDokumen15 halamanAcute Nephritic SyndromeTharen OfficialBelum ada peringkat
- Renal Pathology I. Clinical Manifestations of Renal DiseasesDokumen18 halamanRenal Pathology I. Clinical Manifestations of Renal DiseasesKrisha Marie BadilloBelum ada peringkat
- UTI Dan Glomerular DiseaseDokumen58 halamanUTI Dan Glomerular DiseaseLiana Ika SuwandyBelum ada peringkat
- @acute Nephritic SyndromeDokumen3 halaman@acute Nephritic SyndromeMazlia FarzanaBelum ada peringkat
- Nephritic SyndromeDokumen2 halamanNephritic Syndromevalari8069Belum ada peringkat
- Glomerular 125Dokumen14 halamanGlomerular 125Surgeeth SKBelum ada peringkat
- PATH - Nephritic SyndromeDokumen14 halamanPATH - Nephritic SyndromeMuhamad Zul ImanBelum ada peringkat
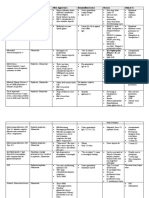
- Differential Diagnosis of Glomerular DiseasesDokumen2 halamanDifferential Diagnosis of Glomerular DiseasesMaryam Fadah100% (1)
- Clinical Approach To: Rapid Progressive GlomerulonephritisDokumen38 halamanClinical Approach To: Rapid Progressive GlomerulonephritisMiri PravdaBelum ada peringkat
- Disease PDFDokumen6 halamanDisease PDFJohn Christopher LucesBelum ada peringkat
- Genetics Table RenalDokumen2 halamanGenetics Table RenalDavid KramerBelum ada peringkat
- Glomerular DiseaseDokumen25 halamanGlomerular DiseaseLeang KarichakBelum ada peringkat
- Disease Key Identification Histology Deposits Nephritic SyndromeDokumen5 halamanDisease Key Identification Histology Deposits Nephritic SyndromeSunny RatnaniBelum ada peringkat
- Medical KidneyDokumen13 halamanMedical KidneyJose SirittBelum ada peringkat
- Revision Notes Chapter 27878 1Dokumen4 halamanRevision Notes Chapter 27878 1Yuku BabyBelum ada peringkat
- Renal DiseaseDokumen5 halamanRenal DiseasefeajhanineladagaBelum ada peringkat
- CompressiveDokumen6 halamanCompressiveyessyBelum ada peringkat
- Humoral and B-Cell Deficiencies PDFDokumen10 halamanHumoral and B-Cell Deficiencies PDFRch 19Belum ada peringkat
- The Table of Frequent Questions - PathologyDokumen14 halamanThe Table of Frequent Questions - PathologyCherry Kola100% (1)
- Nephritic SyndromeDokumen10 halamanNephritic SyndromeRam AryalBelum ada peringkat
- Glomerular Disease and DiureticsDokumen26 halamanGlomerular Disease and DiureticsDapot SianiparBelum ada peringkat
- Systemic Lupus Erythematosus: PathogenesisDokumen5 halamanSystemic Lupus Erythematosus: PathogenesisMiguel Cuevas DolotBelum ada peringkat
- NephriticDokumen6 halamanNephriticAlexandra ChiricencoBelum ada peringkat
- Mediated Disorders: (Type Icrgn) Anti-Glomerular Basement Membrane Antibody Ular Basement Membrane AntibodyDokumen1 halamanMediated Disorders: (Type Icrgn) Anti-Glomerular Basement Membrane Antibody Ular Basement Membrane AntibodyDian Putri NingsihBelum ada peringkat
- Nephrotic Syndrome PDF 2Dokumen2 halamanNephrotic Syndrome PDF 2MBelum ada peringkat
- NEFROPATIA IG A - AndreeaDokumen55 halamanNEFROPATIA IG A - AndreeaSanzianaGogaBelum ada peringkat
- Bagian Patologi Anatomi Fk-Uisu 2011Dokumen22 halamanBagian Patologi Anatomi Fk-Uisu 2011rizapuspairyaniBelum ada peringkat
- Dr. Dhian Endarwati, Spa Maret 2017Dokumen60 halamanDr. Dhian Endarwati, Spa Maret 2017Diany LarasatiBelum ada peringkat
- Nephritic SyndromeDokumen15 halamanNephritic Syndrome76q88b4yrxBelum ada peringkat
- Toronto Notes Nephrology 2015 22Dokumen1 halamanToronto Notes Nephrology 2015 22JUSASB0% (1)
- Glomerulus - SchematicDokumen29 halamanGlomerulus - SchematicNinda NurkhalifahBelum ada peringkat
- Chapter 7Dokumen2 halamanChapter 7Mychelle MenesBelum ada peringkat
- Nephro NotesDokumen4 halamanNephro NotesAliana ABelum ada peringkat
- Gamapatiile Monoclonale PDFDokumen92 halamanGamapatiile Monoclonale PDFJimboreanu György PaulaBelum ada peringkat
- Renal Cheat SheetDokumen3 halamanRenal Cheat Sheetkad ourBelum ada peringkat
- Disorder of Renal System-GnDokumen8 halamanDisorder of Renal System-GnLaxman KannaBelum ada peringkat
- Membranoproliferative GlomerulonephritisDokumen7 halamanMembranoproliferative GlomerulonephritisRobertBelum ada peringkat
- IgA NephropathyDokumen5 halamanIgA NephropathyLara Patricia TamsiBelum ada peringkat
- Journal Club Presentation RPGN-1Dokumen53 halamanJournal Club Presentation RPGN-1sagor9364Belum ada peringkat
- Disorder Etiology: Acute GlomerulonephritisDokumen1 halamanDisorder Etiology: Acute GlomerulonephritisChynna Izzabelle Alcantara AbellanaBelum ada peringkat
- GLOMERULONEPHRITIS (Bright's Disease)Dokumen8 halamanGLOMERULONEPHRITIS (Bright's Disease)Anjitha K. JBelum ada peringkat
- Renal Pathology-1 (Glomerulonephritis) - 2021Dokumen15 halamanRenal Pathology-1 (Glomerulonephritis) - 2021oziad4518Belum ada peringkat
- Chapter 8 - Renal DiseaseDokumen7 halamanChapter 8 - Renal DiseaseCha GuingabBelum ada peringkat
- GlomerulonefritisDokumen8 halamanGlomerulonefritisdhya0303Belum ada peringkat
- Pathology Seminar PPT YASH SARANDokumen22 halamanPathology Seminar PPT YASH SARANYash SaranBelum ada peringkat
- Nephrotic SyndDokumen21 halamanNephrotic Synd238439904Belum ada peringkat
- Glomerular Disease - Dr. LuDokumen8 halamanGlomerular Disease - Dr. LuMACATANGAY, GAELLE LISETTEBelum ada peringkat
- Immuno 9-11Dokumen4 halamanImmuno 9-11Steph TabasaBelum ada peringkat
- 4.2 ImmunodeficiencyDokumen11 halaman4.2 ImmunodeficiencyJohn Anthony de GùzmanBelum ada peringkat
- Immunoglobulin A Nephropathy: Current UpdatesDokumen61 halamanImmunoglobulin A Nephropathy: Current UpdatesRahul PabalkarBelum ada peringkat
- C370 Lecture 2 Lecture Notes Part 2Dokumen45 halamanC370 Lecture 2 Lecture Notes Part 2Yan Mui ChanBelum ada peringkat
- Tracheostomy Suctioning and HumidificationDokumen5 halamanTracheostomy Suctioning and HumidificationLucila LugoBelum ada peringkat
- Clinical Nursing Manual PDFDokumen93 halamanClinical Nursing Manual PDFVatau FlorinBelum ada peringkat
- Prioritization of ProblemDokumen2 halamanPrioritization of ProblemGenette Sy SolisBelum ada peringkat
- Clostridium Difficile Infection and Fecal BacteriotherapyDokumen9 halamanClostridium Difficile Infection and Fecal BacteriotherapyAnonymous nEC4alrPjGBelum ada peringkat
- Community Health Nursing Bag Technique PDFDokumen2 halamanCommunity Health Nursing Bag Technique PDFRachael50% (2)
- Head InjuryDokumen2 halamanHead InjuryHavez KleibBelum ada peringkat
- Pig Heart Dissection Lab 2012-2013finaldraftpdfDokumen21 halamanPig Heart Dissection Lab 2012-2013finaldraftpdfapi-169518406Belum ada peringkat
- The Nursing Assessment Cheat Sheet (ADPIE)Dokumen3 halamanThe Nursing Assessment Cheat Sheet (ADPIE)ajaz100% (1)
- Type 1 DiabetesDokumen8 halamanType 1 DiabetesSam SyawallBelum ada peringkat
- Referat Gangguan Lapang PandangDokumen27 halamanReferat Gangguan Lapang PandangIkrima MuhdarmuhallyBelum ada peringkat
- Respiratory BubblingDokumen7 halamanRespiratory BubblingErwin SiregarBelum ada peringkat
- Guidelines For Acute Care of The Neonate 22eDokumen181 halamanGuidelines For Acute Care of The Neonate 22eKatherin J.Belum ada peringkat
- International Journal of Surgery Case ReportsDokumen4 halamanInternational Journal of Surgery Case Reportshussein_faourBelum ada peringkat
- Neuro 4 5 Penyakit NeurovaskularDokumen27 halamanNeuro 4 5 Penyakit NeurovaskularHalima TusadiaBelum ada peringkat
- PFP Bedboard User GuideDokumen87 halamanPFP Bedboard User GuideSrinivas BhupathiBelum ada peringkat
- SAMPLE FDAR CHARTING PainDokumen1 halamanSAMPLE FDAR CHARTING Painjpm100% (1)
- H02E Assignment 8Dokumen4 halamanH02E Assignment 8Good ChannelBelum ada peringkat
- Clinical Approach To Rapidly Progressive Renal FailureDokumen6 halamanClinical Approach To Rapidly Progressive Renal FailureBryan RamseyBelum ada peringkat
- 98 Painad PDFDokumen2 halaman98 Painad PDFmaKitten08Belum ada peringkat
- Admission Note TemplateDokumen4 halamanAdmission Note TemplateTauhid Mahmud100% (2)
- (Mahesh Chandra) Objective Cardiology PDFDokumen609 halaman(Mahesh Chandra) Objective Cardiology PDFfajarBelum ada peringkat
- Diagnosis of Adjustment Disorder Reliability of Its Clinical Use and Long-Term StabilityDokumen6 halamanDiagnosis of Adjustment Disorder Reliability of Its Clinical Use and Long-Term StabilitydmsdsBelum ada peringkat
- Anticoagulants 2019Dokumen11 halamanAnticoagulants 2019Srijan VermaBelum ada peringkat
- Acute and Chronic Gastritis Due To Helicobacter PyloriDokumen8 halamanAcute and Chronic Gastritis Due To Helicobacter PyloriCarla HolandBelum ada peringkat
- Document DRUG 4Dokumen4 halamanDocument DRUG 4Linda AdamsonBelum ada peringkat
- Drug Tariff Workshop 13-14 - StudentDokumen10 halamanDrug Tariff Workshop 13-14 - StudentCrystal Sia Yiik SwanBelum ada peringkat
- Perfil Neuropsicologico Paciente Cirrosis Paez 2011Dokumen21 halamanPerfil Neuropsicologico Paciente Cirrosis Paez 2011catalinaBelum ada peringkat
- Final Exam: Theory of Nursing SystemsDokumen2 halamanFinal Exam: Theory of Nursing SystemsXeian Calamba RafaelBelum ada peringkat
- GNU HealthDokumen1 halamanGNU Healthbhupendrapawar279Belum ada peringkat