Anda mungkin juga menyukai
- Diagnosis Dan Diagnosis Banding DM SK 2Dokumen99 halamanDiagnosis Dan Diagnosis Banding DM SK 2syahron maskatBelum ada peringkat
- Daftar Pustaka Hipertensi Pada Usia MudaDokumen10 halamanDaftar Pustaka Hipertensi Pada Usia MudaToby Hadinata WiranegaraBelum ada peringkat
- Manajemen HipertensiDokumen46 halamanManajemen HipertensiYeni BelawatiBelum ada peringkat
- Referat Diare Pada AnakDokumen45 halamanReferat Diare Pada AnakNaily HosenBelum ada peringkat
- Resusitasi Jantung Paru Berkualitas: Dr. Ichwan Zuanto 3 FEBRUARI 2018 Rsia Setya BhaktiDokumen12 halamanResusitasi Jantung Paru Berkualitas: Dr. Ichwan Zuanto 3 FEBRUARI 2018 Rsia Setya BhaktiIchwan Zuanto SjamanBelum ada peringkat
- IHR-Travel MedicineDokumen45 halamanIHR-Travel MedicineEndang Sri LestariBelum ada peringkat
- Preeklampsia: Tata Laksana TerkiniDokumen50 halamanPreeklampsia: Tata Laksana TerkiniSRI WIDOWATIBelum ada peringkat
- Combustio Grade II A + BDokumen16 halamanCombustio Grade II A + BDyna Eka AlphattinsonBelum ada peringkat
- FL Leaflet Napza FixDokumen2 halamanFL Leaflet Napza FixDesii NainggolanBelum ada peringkat
- Left Ventricular Hyperthrophy CriteriaDokumen2 halamanLeft Ventricular Hyperthrophy CriteriaDya AndryanBelum ada peringkat
- Eklampsia 1Dokumen10 halamanEklampsia 1Zulvikar MatikeBelum ada peringkat
- SOP Cutaneus Larva Migran 1Dokumen2 halamanSOP Cutaneus Larva Migran 1Muhammad IqbalBelum ada peringkat
- Pedoman SurveilansDokumen24 halamanPedoman Surveilanskadek macelino100% (1)
- Hubungan Preeklamsi Berat Dengan Kelahiran PretermDokumen10 halamanHubungan Preeklamsi Berat Dengan Kelahiran PretermVera Andri YaniBelum ada peringkat
- RPT-IMD-ASIDokumen15 halamanRPT-IMD-ASIabdul halikBelum ada peringkat
- Gastric Ulcer ReviewDokumen6 halamanGastric Ulcer Reviewshanthi dasariBelum ada peringkat
- PosterDokumen1 halamanPosterNdha Nezz WoanBelum ada peringkat
- LABIOPALATOSCHIZISDokumen25 halamanLABIOPALATOSCHIZISEya Prepti SerraBelum ada peringkat
- Poa Ispa 2020Dokumen34 halamanPoa Ispa 2020ugdBelum ada peringkat
- (MNTP) Materi - Psikiatri PDFDokumen146 halaman(MNTP) Materi - Psikiatri PDFNatasha Enid StefanieBelum ada peringkat
- Leaflet Demam BerdarahDokumen2 halamanLeaflet Demam BerdarahbbBelum ada peringkat
- Daftar Pustaka StuntingDokumen1 halamanDaftar Pustaka StuntingtomoandiBelum ada peringkat
- Pedoman TBDokumen59 halamanPedoman TBSukma Dewi SimamoraBelum ada peringkat
- Pelaporan IKP Puskesmas Arjaty Daud 2022Dokumen16 halamanPelaporan IKP Puskesmas Arjaty Daud 2022Fajar Slalu CeriaBelum ada peringkat
- Tabel Referensi Diagnosa Non SpesialistikDokumen12 halamanTabel Referensi Diagnosa Non SpesialistikDian SunartiBelum ada peringkat
- Hubungan Stres Dengan Kualitas Hidup Penderita Diabetes Mellitus Tipe 2Dokumen9 halamanHubungan Stres Dengan Kualitas Hidup Penderita Diabetes Mellitus Tipe 2Wirda RinaBelum ada peringkat
- Dosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDokumen1 halamanDosis Obat Premedikasi: No Golongan Nama Obat Dosis Dewasa (MG) Dosis Anak RuteDenny RamdhanBelum ada peringkat
- Icd 10 $Dokumen31 halamanIcd 10 $rahmiatiBelum ada peringkat
- Pekerjaan Kode Unit Kerja D6205Dokumen466 halamanPekerjaan Kode Unit Kerja D6205Irfansyah MaladiBelum ada peringkat
- Kepatuhan Minum Obat Pada Paien TB ParuDokumen14 halamanKepatuhan Minum Obat Pada Paien TB ParuFaishol IriyantoBelum ada peringkat
- Demam TifoidDokumen32 halamanDemam TifoidMageswari SelvarajooBelum ada peringkat
- Material Safety Data Sheet: AseptanDokumen5 halamanMaterial Safety Data Sheet: AseptanfitrinuraniBelum ada peringkat
- Penatalaksanaan DiabetesDokumen63 halamanPenatalaksanaan DiabetesNikma ayuniBelum ada peringkat
- TB Paru FK UncenDokumen66 halamanTB Paru FK UncenAndira Trianingrum TukanBelum ada peringkat
- HepatitisDokumen39 halamanHepatitisDocRN50% (2)
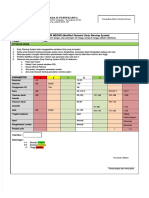
- Formulir Meows (FORMULIR MEOWS (Modified Obstetric Early Warning System Modified Obstetric Early Warning System) )Dokumen2 halamanFormulir Meows (FORMULIR MEOWS (Modified Obstetric Early Warning System Modified Obstetric Early Warning System) )miraBelum ada peringkat
- MAKALAH Artikel Asi EksklusifDokumen4 halamanMAKALAH Artikel Asi EksklusifMegumiaisyahBelum ada peringkat
- Status Kunjungan Puskesmas Ibrahim AdjieDokumen1 halamanStatus Kunjungan Puskesmas Ibrahim Adjieelka kurniaBelum ada peringkat
- Medical Check Up: Cek KesehatanDokumen20 halamanMedical Check Up: Cek KesehatanEmi PephiBelum ada peringkat
- Managing Hypertension in the ElderlyDokumen88 halamanManaging Hypertension in the ElderlyMuzayyanatulhayat ARBelum ada peringkat
- Aqcuired Immunodeficiency SyndromeDokumen78 halamanAqcuired Immunodeficiency SyndromeandiariansyahBelum ada peringkat
- ID Faktor Faktor Yang Mempengaruhi PerilakuDokumen11 halamanID Faktor Faktor Yang Mempengaruhi PerilakuM Ekmal Yusuf PutraBelum ada peringkat
- Penyebabnya VIRUS Dengue: DEN-1, DEN-2, DEN-3, DEN-4. Ditularkan Lewat Gigitan Nyamuk AEDESDokumen41 halamanPenyebabnya VIRUS Dengue: DEN-1, DEN-2, DEN-3, DEN-4. Ditularkan Lewat Gigitan Nyamuk AEDESarischarompisBelum ada peringkat
- Makanan Tambahan Pada Anak: Apa Itu Gizi???Dokumen2 halamanMakanan Tambahan Pada Anak: Apa Itu Gizi???annisaBelum ada peringkat
- Diabetes Mellitus 2017Dokumen149 halamanDiabetes Mellitus 2017Rani BenawaBelum ada peringkat
- Refreshing DHFDokumen13 halamanRefreshing DHFNia Nurhayati ZakiahBelum ada peringkat
- Abses Mammae - Gesti Pratiwi HPDokumen17 halamanAbses Mammae - Gesti Pratiwi HPYobbi ArissaputraBelum ada peringkat
- UPTD Puskesmas Pinolosian Glasgow Coma Scale and Burn Wound TreatmentDokumen42 halamanUPTD Puskesmas Pinolosian Glasgow Coma Scale and Burn Wound TreatmentNi Made Trisnawati100% (1)
- Program Prolanis: Kelompok 3Dokumen48 halamanProgram Prolanis: Kelompok 3Hardian DwiBelum ada peringkat
- Stimulasi Kader Kelompok Sayang Ibu Tentang ANC, ASI Eksklusif, KB dan ImunisasiDokumen102 halamanStimulasi Kader Kelompok Sayang Ibu Tentang ANC, ASI Eksklusif, KB dan Imunisasial furqonBelum ada peringkat
- Hemoroid Interna Laporan KasusDokumen4 halamanHemoroid Interna Laporan KasusSarah Humaira DennisonBelum ada peringkat
- Label 103Dokumen1 halamanLabel 103Umar DhaniBelum ada peringkat
- MSDS Ziehl Neelsen 2Dokumen3 halamanMSDS Ziehl Neelsen 2lab RSUDPameungpeukBelum ada peringkat
- Cara Hitung Jasa JKNDokumen4 halamanCara Hitung Jasa JKNmuhammad iqbalBelum ada peringkat
- Sindrom Nefritik DebDokumen2 halamanSindrom Nefritik DebrchristevenBelum ada peringkat
- Pelayanan Ramah Anak Di PuskesmasDokumen28 halamanPelayanan Ramah Anak Di Puskesmasdinas kesehatanBelum ada peringkat
- Leaflet IspaDokumen3 halamanLeaflet Ispanurindah tri wBelum ada peringkat
- Diabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMDokumen20 halamanDiabetes Mellitus: Salient Features of Type 1 Am D Type 2 DMPriyanka Karnik100% (1)
- Diabetes MelitusDokumen57 halamanDiabetes MelitusArzyad Analis KesehatanBelum ada peringkat
- Diabetes Mellitus Final SibiDokumen62 halamanDiabetes Mellitus Final SibiSibi JohnBelum ada peringkat
- CyclamenDokumen9 halamanCyclamenLAUM1Belum ada peringkat
- Pre Miro Lab LesDokumen3 halamanPre Miro Lab Lesrain rainyBelum ada peringkat
- Nur 097 Sas 1 3Dokumen9 halamanNur 097 Sas 1 3gekkonoojiBelum ada peringkat
- Laser: DR Uzair Ahmad Qureshi Consultant Dermatologist, STDS, Laser and Aesthetic SpecialistDokumen18 halamanLaser: DR Uzair Ahmad Qureshi Consultant Dermatologist, STDS, Laser and Aesthetic SpecialistFakhra TehseenBelum ada peringkat
- 2023061-21 Seminar On The Development and Application of Mobile PaymentDokumen3 halaman2023061-21 Seminar On The Development and Application of Mobile PaymentMunkhuu NasaaBelum ada peringkat
- Pug BookDokumen152 halamanPug BookArtemio SotomayorBelum ada peringkat
- F7.6 Seafarers Medical Examination-CertificateDokumen7 halamanF7.6 Seafarers Medical Examination-CertificateHerbert Maganga100% (1)
- MeningitisDokumen21 halamanMeningitisSonya GodwinBelum ada peringkat
- 3 Ceramic Pot Water FilterDokumen32 halaman3 Ceramic Pot Water Filtermohammed abdellaBelum ada peringkat
- ABG AnalysisDokumen15 halamanABG AnalysisPabhat Kumar100% (2)
- A Novel Technique For Pudendal Nerve BlockDokumen4 halamanA Novel Technique For Pudendal Nerve Blockmohs2007100% (1)
- Nursing Diagnosis For AsthmaDokumen6 halamanNursing Diagnosis For AsthmaTINAIDA33% (3)
- 15 Immunogenetics-89402Dokumen34 halaman15 Immunogenetics-89402SunuBelum ada peringkat
- Pediatrics ImpDokumen233 halamanPediatrics Impملك عيسى100% (1)
- Fall 2010 Eco Newsletter, EcoSuperiorDokumen12 halamanFall 2010 Eco Newsletter, EcoSuperiorEco SuperiorBelum ada peringkat
- Rapyuta Robotics PVT LTD - GMC Renewal Quote - 28th Dec2022Dokumen1 halamanRapyuta Robotics PVT LTD - GMC Renewal Quote - 28th Dec2022nagarajgnairyBelum ada peringkat
- Psychosis ObjectivesDokumen14 halamanPsychosis ObjectivesfatenBelum ada peringkat
- Chapter 7 Africa South of The SaharaDokumen40 halamanChapter 7 Africa South of The Saharafuck ypouBelum ada peringkat
- Pharmacy SyllabusDokumen89 halamanPharmacy SyllabusDivvela ManoharBelum ada peringkat
- Important Uses of Neem ExtractDokumen3 halamanImportant Uses of Neem ExtractAbdurrahman MustaphaBelum ada peringkat
- MalariaDokumen4 halamanMalarianafrabBelum ada peringkat
- AllergiesDokumen11 halamanAllergiesAficionadoBelum ada peringkat
- Food PreparationDokumen127 halamanFood PreparationRUMBIDZAI MELLISA DZINZIBelum ada peringkat
- Physical Paper +1ANNUALDokumen5 halamanPhysical Paper +1ANNUALprabhnoorprimeBelum ada peringkat
- Folk Biology and The Anthropology of Science Cognitive Universals and Cultural ParticularsDokumen63 halamanFolk Biology and The Anthropology of Science Cognitive Universals and Cultural ParticularsGaby ArguedasBelum ada peringkat
- Biological Science Reviewer QuestionsDokumen14 halamanBiological Science Reviewer QuestionsRavian Mhe BitonBelum ada peringkat
- Disease Prediction Using Machine LearningDokumen10 halamanDisease Prediction Using Machine LearningIJRASETPublicationsBelum ada peringkat
- Trilobata Exhibits Molecular Impediment On TheDokumen10 halamanTrilobata Exhibits Molecular Impediment On TheInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Physical Education Mcqs For All Govt ExamDokumen108 halamanPhysical Education Mcqs For All Govt Examrabiaghafar855Belum ada peringkat
- ZZZZZZZZZZZZZZDokumen8 halamanZZZZZZZZZZZZZZchloramphenicolBelum ada peringkat