Anda mungkin juga menyukai
- How To Interpret Thyroid Function TestDokumen5 halamanHow To Interpret Thyroid Function TestSiveshKathirKamarajahBelum ada peringkat
- HYPOTHYROIDISMDokumen30 halamanHYPOTHYROIDISMTopeBelum ada peringkat
- Chapter - 2 Hypothyroidism de Overcoming Thyroid Disorders PDFDokumen35 halamanChapter - 2 Hypothyroidism de Overcoming Thyroid Disorders PDFsantana2007Belum ada peringkat
- Hypo Thyroid Is MDokumen3 halamanHypo Thyroid Is MjhBelum ada peringkat
- Hypothalamic Pitutary Axis and Thyroid Hormone SynthesisDokumen5 halamanHypothalamic Pitutary Axis and Thyroid Hormone Synthesis78 shivangi mauryaBelum ada peringkat
- Thyroid Emergencies-Dr. AM IyagbaDokumen13 halamanThyroid Emergencies-Dr. AM IyagbaDr. Amb. Monday ZaccheausBelum ada peringkat
- Thyroid DX PXLDokumen62 halamanThyroid DX PXLabduljebarBelum ada peringkat
- Thyroid Disorders During PregnancyDokumen25 halamanThyroid Disorders During PregnancyA.H.ABelum ada peringkat
- Endocrine 160110083024Dokumen65 halamanEndocrine 160110083024Ryan CracknellBelum ada peringkat
- Hyperthyroidsm: EpidemiologyDokumen6 halamanHyperthyroidsm: EpidemiologyEllieBelum ada peringkat
- Adrenocortical HyperfunctionDokumen132 halamanAdrenocortical Hyperfunctionshobharamkrishna100% (2)
- Hypothyroid in Pregnancy Andi CakraDokumen32 halamanHypothyroid in Pregnancy Andi CakraCakraEkkyBelum ada peringkat
- The Nutritional Relationships of MagnesiumDokumen5 halamanThe Nutritional Relationships of MagnesiumwynvelBelum ada peringkat
- Hypothyroidism in PregnancyDokumen14 halamanHypothyroidism in PregnancyShajia ZafarBelum ada peringkat
- Thyroid and InfertilityDokumen36 halamanThyroid and InfertilitySairindri SahooBelum ada peringkat
- Week 3 Pharmaco Part 2Dokumen34 halamanWeek 3 Pharmaco Part 2Tiko JomidavaBelum ada peringkat
- Abnormal Thyroid Function in PregnancyDokumen54 halamanAbnormal Thyroid Function in Pregnancyasri khazaliBelum ada peringkat
- Psychiatric Effects of ThyroidDokumen9 halamanPsychiatric Effects of ThyroidJosetta WhitneyBelum ada peringkat
- Laboratory Diagnostics of (Selected) Endocrine DisordersDokumen48 halamanLaboratory Diagnostics of (Selected) Endocrine DisordersPaulina PaskeviciuteBelum ada peringkat
- FunctionTests Brochure PDFDokumen2 halamanFunctionTests Brochure PDFArslan SaleemBelum ada peringkat
- Thyroid Function Tests (TFTS)Dokumen27 halamanThyroid Function Tests (TFTS)ธิติวุฒิ แสงคล้อยBelum ada peringkat
- Thyroid HormoneDokumen396 halamanThyroid HormoneuiliftengBelum ada peringkat
- Biol 460 Case StudyDokumen11 halamanBiol 460 Case Studyapi-353888678Belum ada peringkat
- A Quick Guide To HypoparathyroidismDokumen24 halamanA Quick Guide To HypoparathyroidismCota AncutaBelum ada peringkat
- Pemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKDokumen12 halamanPemeriksaaan Laboratorium Kelainan Thyroid: DR - Budi Dermawan Lubis, SPPK DR - Siti Hajar, M.Ked, SPPKBonitavanyBelum ada peringkat
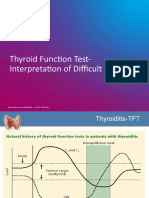
- TFT Interpretation of Difficult CasesDokumen51 halamanTFT Interpretation of Difficult CasesAditya GautamBelum ada peringkat
- Thyroid HormonesDokumen7 halamanThyroid HormonesAbdullah EssaBelum ada peringkat
- Graves' Hyperthyroidism in Pregnancy: A Clinical ReviewDokumen22 halamanGraves' Hyperthyroidism in Pregnancy: A Clinical ReviewAnisa Dinda NurlianaBelum ada peringkat
- Thyroid Function Test: The "Hidden" Health ProblemDokumen34 halamanThyroid Function Test: The "Hidden" Health Problemvjanand07100% (1)
- Laboratory Tests of Thyroid Function: Uses and Limitations: D. Robert Dufour, MDDokumen16 halamanLaboratory Tests of Thyroid Function: Uses and Limitations: D. Robert Dufour, MDStacy SmithBelum ada peringkat
- Thyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneDokumen41 halamanThyroid Disease: Presentation By: Pimundu Vicent Audo Ritah Tutor: Dr. Fualal JaneEsther AumaBelum ada peringkat
- Gds137 Slide HyperthyroidismDokumen30 halamanGds137 Slide HyperthyroidismLouie Kem Anthony BabaranBelum ada peringkat
- Lipoprotein & Dyslipidemia DR Lin Oswari Blok 8Dokumen97 halamanLipoprotein & Dyslipidemia DR Lin Oswari Blok 8Izzah AtqaBelum ada peringkat
- Grave'S Disease: Farida Ulfa 1510211057Dokumen11 halamanGrave'S Disease: Farida Ulfa 1510211057farida ulfaBelum ada peringkat
- Thyroid AntibodiesDokumen31 halamanThyroid AntibodiesCharlesAntonypillaiBelum ada peringkat
- The Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornDokumen36 halamanThe Role of Maternal Thyroid Status On Pregnancy Outcome For Motherand NewbornRahmayantiYuliaBelum ada peringkat
- Hormon GDSDokumen23 halamanHormon GDSBRI KUBelum ada peringkat
- Thyroid Function TestDokumen28 halamanThyroid Function TestDhinesh Muthusamy100% (1)
- Adrenal Insufficiency and Cushing's Disease-1Dokumen34 halamanAdrenal Insufficiency and Cushing's Disease-1Mwanja MosesBelum ada peringkat
- How To Interpret Thyroid Function TestsDokumen5 halamanHow To Interpret Thyroid Function TestsnonieshzBelum ada peringkat
- Thyroiddisease 190216062020Dokumen42 halamanThyroiddisease 190216062020Manikandan Vp100% (1)
- Thyroid DisordersDokumen29 halamanThyroid DisordersEMPIBelum ada peringkat
- The King and The 2006 Coup by Kevin HewisonDokumen22 halamanThe King and The 2006 Coup by Kevin HewisonZuzen JusticeBelum ada peringkat
- Thyroid Function TestsDokumen21 halamanThyroid Function TestsPraneeth TirumalasettyBelum ada peringkat
- Male Hypogonadism: EAU Guidelines OnDokumen34 halamanMale Hypogonadism: EAU Guidelines OnAyu sri WidianiBelum ada peringkat
- Clinical Science HashimotoDokumen36 halamanClinical Science HashimotoImartaBelum ada peringkat
- Thyroid Storm: (Krisis Tiroid)Dokumen17 halamanThyroid Storm: (Krisis Tiroid)BonitavanyBelum ada peringkat
- Thyroid Drug and Calcium Homeostasis - PHD332 - 30112017Dokumen62 halamanThyroid Drug and Calcium Homeostasis - PHD332 - 30112017Alisa BoonsukBelum ada peringkat
- Hyperthyroidism (Thyrotoxicosis) : 郑州大学第一附院内分泌科 王守俊 Wang shou junDokumen133 halamanHyperthyroidism (Thyrotoxicosis) : 郑州大学第一附院内分泌科 王守俊 Wang shou junapi-19916399Belum ada peringkat
- Actions of Thyroid Hormone: Dr. Ayisha Qureshi Assistant Professor MBBS, MphilDokumen41 halamanActions of Thyroid Hormone: Dr. Ayisha Qureshi Assistant Professor MBBS, MphilJyoti ChadhaBelum ada peringkat
- Thyroid DrugsDokumen6 halamanThyroid DrugsThe Real UploaderBelum ada peringkat
- Lactose IntoleranceDokumen19 halamanLactose IntolerancehafeezmmlBelum ada peringkat
- HypertyroidismDokumen46 halamanHypertyroidismenriBelum ada peringkat
- Even If You Eat Perfectly, Not Knowing This Could Leave You DepressedDokumen5 halamanEven If You Eat Perfectly, Not Knowing This Could Leave You DepressedzaskribdoBelum ada peringkat
- Clinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Dokumen63 halamanClinical Practice Guidelines For Hypothyroidism in Adults: AACE and ATA 2012Nur Rakhma AkmaliaBelum ada peringkat
- Thyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistDokumen30 halamanThyroid Disease: Dr. Gusti Hariyadi Maulana, MSC, SPPD-KGH Internist-NephrologistNurul HikmaBelum ada peringkat
- TPO in PregnancyDokumen18 halamanTPO in PregnancyRoxana TudorBelum ada peringkat
- Myelodysplastic SyndromeDokumen20 halamanMyelodysplastic SyndrometeamstrocaBelum ada peringkat
- Thyroid Emergencies: Abrar AlharbiDokumen35 halamanThyroid Emergencies: Abrar AlharbiabrarBelum ada peringkat
- ENDOCRINOLOGY Notes 2 PDFDokumen131 halamanENDOCRINOLOGY Notes 2 PDFkomal pattabiBelum ada peringkat
- Management of Graves Disease 2015 JAMA ADokumen11 halamanManagement of Graves Disease 2015 JAMA AMade ChandraBelum ada peringkat
- The Clinical Significance of Subclinical Thyroid Dysfunction Bernadette Biondi and David S. Cooper PDFDokumen56 halamanThe Clinical Significance of Subclinical Thyroid Dysfunction Bernadette Biondi and David S. Cooper PDFLorena IbarrolaBelum ada peringkat
- Thyroid HormonesDokumen6 halamanThyroid Hormonesحوراء عارف الموسويBelum ada peringkat
- HyperthyroidismDokumen18 halamanHyperthyroidismWahyuni FatmonaBelum ada peringkat
- English Sistem EndocrineDokumen9 halamanEnglish Sistem EndocrineNurlaili YaniBelum ada peringkat
- Metabolic Effects of 3,5-Diiodo-L-Thyronine Giammanco M Et AlDokumen11 halamanMetabolic Effects of 3,5-Diiodo-L-Thyronine Giammanco M Et AlMarco GiammancoBelum ada peringkat
- Sustained Release T3 TherapyDokumen10 halamanSustained Release T3 TherapyKARISHMA SHAIKHBelum ada peringkat
- Case Study - Toxic GoiterDokumen22 halamanCase Study - Toxic GoiterJohn Matley Caampued100% (2)
- Hormonal Response To ExerciseDokumen44 halamanHormonal Response To ExerciseMuhammad shayan umarBelum ada peringkat
- Graves DiseaseDokumen8 halamanGraves Diseasenini07Belum ada peringkat
- Meta BalanceDokumen19 halamanMeta BalancetstaevaBelum ada peringkat
- Thyroid Disorder NCPDokumen9 halamanThyroid Disorder NCPKen RegalaBelum ada peringkat
- Anatomy. Case Study. It's Just StressDokumen4 halamanAnatomy. Case Study. It's Just Stressjonar parinasBelum ada peringkat
- 1 Anatomy and Physiology of Farm AnimalsDokumen251 halaman1 Anatomy and Physiology of Farm AnimalsErin MontillanoBelum ada peringkat
- Understanding Your Lab Tests: ChemistryDokumen13 halamanUnderstanding Your Lab Tests: ChemistryAnalyn SarmientoBelum ada peringkat
- Chapter 45 Hormones and The Endocrine SystemDokumen12 halamanChapter 45 Hormones and The Endocrine System蔡旻珊Belum ada peringkat
- Review Article: Autoimmune Thyroid DisordersDokumen10 halamanReview Article: Autoimmune Thyroid DisordersBJ DixBelum ada peringkat
- 003 FT3-en-EU-V8.1Dokumen4 halaman003 FT3-en-EU-V8.1Jose Adán Abdala PalmaBelum ada peringkat
- All About Thyroid 2019Dokumen45 halamanAll About Thyroid 2019Octo IndradjajaBelum ada peringkat
- Iodine Deficiency DisordersDokumen7 halamanIodine Deficiency DisordersEndocrinology IndiaBelum ada peringkat
- Endocrine Notes (Harrisons)Dokumen27 halamanEndocrine Notes (Harrisons)Valerie Gonzaga-CarandangBelum ada peringkat
- Nursing Hyperthyroidism Study GuideDokumen4 halamanNursing Hyperthyroidism Study GuideLin SookdeeBelum ada peringkat
- How NAC and Glutathione Can Help To Heal Hashimoto's DiseaseDokumen4 halamanHow NAC and Glutathione Can Help To Heal Hashimoto's Diseasemightyfever2973Belum ada peringkat
- HypothyroidismDokumen15 halamanHypothyroidismfachrulmirzaBelum ada peringkat
- HA 1 - Head, Face, Neck, Lymphatic - Student Version 6 Slides Per PageDokumen2 halamanHA 1 - Head, Face, Neck, Lymphatic - Student Version 6 Slides Per Pagegifty rathaurBelum ada peringkat
- Thyroid Disorders TBL Pathology Learning MaterialDokumen20 halamanThyroid Disorders TBL Pathology Learning MaterialIrdina SyabilBelum ada peringkat
- Enf Tiroidea y Embarazo Lancet 2018Dokumen12 halamanEnf Tiroidea y Embarazo Lancet 2018Jair Alexander Quintero PanucoBelum ada peringkat
- IEC Presentation PintuDokumen25 halamanIEC Presentation PintuPintu MahtoBelum ada peringkat
- Fasting and Thyroid Test ResultsDokumen4 halamanFasting and Thyroid Test ResultsRosBelum ada peringkat