Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Pre-Intermediate English: Review 2 (UNITS 13-23) : Grammar: The PastDokumen11 halamanPre-Intermediate English: Review 2 (UNITS 13-23) : Grammar: The PastPaula Correia AraujoBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- This Is The BBC Top 200 BooksDokumen7 halamanThis Is The BBC Top 200 Booksyubel100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Organic Chicken RaisingDokumen24 halamanOrganic Chicken RaisingBonie Jay Mateo Dacot100% (2)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- My Small and Large Intestines: © Teacher Created Resources, Inc. #211 My BodyDokumen3 halamanMy Small and Large Intestines: © Teacher Created Resources, Inc. #211 My Bodyalana reneBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Fluency SentencesDokumen137 halamanFluency Sentencesppy2011100% (2)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Andrew Loomis - Successful DrawingDokumen211 halamanAndrew Loomis - Successful Drawingdiogo.chagas02Belum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- To Be Accomplished by The Licensed Manning Agency.: Repatriation Information Sheet 2Dokumen1 halamanTo Be Accomplished by The Licensed Manning Agency.: Repatriation Information Sheet 2ian clark MarinduqueBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- D - Amico - Functional Occlusion of The Natural Teeth of ManDokumen17 halamanD - Amico - Functional Occlusion of The Natural Teeth of ManMeidad ChassidBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- AnalogyDokumen94 halamanAnalogyRizwan KhanBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Gayatri Mantra MudraDokumen3 halamanGayatri Mantra Mudradineshgomber100% (1)
- Eskimo (Inuit) MagicDokumen4 halamanEskimo (Inuit) MagicPaganlady100% (1)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Osteology - Anatomical Orientations, Planes, DirectionsDokumen74 halamanOsteology - Anatomical Orientations, Planes, DirectionsCagatay BarutBelum ada peringkat
- Guidelines For Combi-OvensDokumen9 halamanGuidelines For Combi-OvensDavid BradleyBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Tai Chi Breathing PDFDokumen11 halamanTai Chi Breathing PDFAYDE100% (2)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Reading Comprehension WorkbookDokumen27 halamanReading Comprehension WorkbookKristina AlaverdyanBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Blood 12-6-2018Dokumen42 halamanBlood 12-6-2018Noor Fatima100% (1)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Answers Eng G5 2020Dokumen27 halamanAnswers Eng G5 2020Neel BCBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Animal Genetics and BreedingDokumen2 halamanAnimal Genetics and BreedingNewtonBelum ada peringkat
- AV3 - SpeakingDokumen11 halamanAV3 - SpeakingHuân MinhBelum ada peringkat
- Dairy 2 PDFDokumen23 halamanDairy 2 PDFSariful IslamBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- BrerRabbit PDFDokumen15 halamanBrerRabbit PDFantonapoulosBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Acne Vulgaris: Abdul Alraiyes 5/7/08Dokumen22 halamanAcne Vulgaris: Abdul Alraiyes 5/7/08Abdul Hamid AlraiyesBelum ada peringkat
- Evaluación Física y Clínica de Sementales Bovinos en Dos Municipios de La Costa Chica de Guerrero, MéxicoDokumen7 halamanEvaluación Física y Clínica de Sementales Bovinos en Dos Municipios de La Costa Chica de Guerrero, MéxicoChacharitas IxtapalucachalcoBelum ada peringkat
- EDLDokumen2 halamanEDLHannahBelum ada peringkat
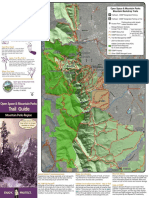
- Trail Guide: Open Space & Mountain ParksDokumen2 halamanTrail Guide: Open Space & Mountain ParksKeith GruberBelum ada peringkat
- Natural Selection PowerpointDokumen7 halamanNatural Selection Powerpointapi-202513022Belum ada peringkat
- Physioanatomical Explanation of Abhyanga An Ayurvedic Massagetechnique For Healthy LifeDokumen5 halamanPhysioanatomical Explanation of Abhyanga An Ayurvedic Massagetechnique For Healthy LifeverenagarciaBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Anatomy Unit 4 Skin and Body MembranesDokumen45 halamanAnatomy Unit 4 Skin and Body MembranesJaren BalbalBelum ada peringkat
- Essay HivDokumen8 halamanEssay Hivapi-271273976Belum ada peringkat
- Felix Und FranziDokumen102 halamanFelix Und FranziDana Nanu100% (1)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)