Anda mungkin juga menyukai
- Kuliah Gangguan Pertumbuhan PBLDokumen43 halamanKuliah Gangguan Pertumbuhan PBLGistaBelum ada peringkat
- Referat Pertumbuhan Aloisia DysiDokumen34 halamanReferat Pertumbuhan Aloisia DysiAloisia DysiBelum ada peringkat
- Perawakan Pendek: Etiologi, Diagnosis dan TatalaksanaDokumen18 halamanPerawakan Pendek: Etiologi, Diagnosis dan TatalaksanaTri Utami Wahyuningsih100% (1)
- PerawakanPendekDokumen17 halamanPerawakanPendekDyan LihawaBelum ada peringkat
- Pertumbuhan LinierDokumen45 halamanPertumbuhan LinierSi Puput100% (1)
- KOKPENDEKDokumen17 halamanKOKPENDEKAldy GeriBelum ada peringkat
- PERTAMAHAN PERTUMBUHANDokumen8 halamanPERTAMAHAN PERTUMBUHANIbam Bukan IkanBelum ada peringkat
- Perawakan Tinggi: Heightisme, Perawakan Tinggi Bukan Merupakan Keluhan Biasa. Perawakan Tinggi Bisa MerupakanDokumen16 halamanPerawakan Tinggi: Heightisme, Perawakan Tinggi Bukan Merupakan Keluhan Biasa. Perawakan Tinggi Bisa MerupakanguptaBelum ada peringkat
- PERAWAKAN PENDEKDokumen29 halamanPERAWAKAN PENDEKFara OmarBelum ada peringkat
- Perawakan PendekDokumen37 halamanPerawakan PendekMyra Marianty100% (2)
- Perawakan PendekDokumen36 halamanPerawakan PendekKhanif Kinesthesia CahyagamaBelum ada peringkat
- Perawakan Pendek Pada AnakDokumen4 halamanPerawakan Pendek Pada AnakNur Azizah Noviyana SBelum ada peringkat
- Aman PulunganDokumen8 halamanAman PulunganweisenheimBelum ada peringkat
- (ADT) Pertumbuhan Dan PubertasDokumen96 halaman(ADT) Pertumbuhan Dan PubertasfitriBelum ada peringkat
- Perawakan PendekDokumen9 halamanPerawakan PendekHerlina ElinBelum ada peringkat
- Pertumbuhan Dan Gangguan PertumbuhanDokumen9 halamanPertumbuhan Dan Gangguan PertumbuhanPratiwi N. TanioBelum ada peringkat
- ShortstatureDokumen32 halamanShortstatureRizki PratamaBelum ada peringkat
- Growth Hormon DemarDokumen21 halamanGrowth Hormon DemarDemar BerkamBelum ada peringkat
- SKENARIO DDokumen21 halamanSKENARIO DSarah SilaenBelum ada peringkat
- StuntingDokumen7 halamanStuntingratna kartikaBelum ada peringkat
- Terapi Hormon Pertumbuhan Untuk Anak Lahir Kecil Masa KehamilanDokumen12 halamanTerapi Hormon Pertumbuhan Untuk Anak Lahir Kecil Masa KehamilanAlmira Aliyannisa PattisahusiwaBelum ada peringkat
- Patofisiologi Stunting - CompressedDokumen26 halamanPatofisiologi Stunting - CompressedNers 2022Belum ada peringkat
- Gangguan Pubertas ShandyDokumen47 halamanGangguan Pubertas ShandyShandy Suwanto Putra100% (3)
- Cegah StuntingDokumen33 halamanCegah StuntingsriBelum ada peringkat
- Nutritional Management of Stunting in Children (Endang Lestari)Dokumen37 halamanNutritional Management of Stunting in Children (Endang Lestari)FitriaBelum ada peringkat
- PBL Blok 21Dokumen17 halamanPBL Blok 21Anonymous ntIaRgBelum ada peringkat
- Terlambat Pubertas: Penyebab, Gejala, Diagnosis dan PenanganannyaDokumen17 halamanTerlambat Pubertas: Penyebab, Gejala, Diagnosis dan PenanganannyaFathur RahmanBelum ada peringkat
- Perawakan TinggiDokumen3 halamanPerawakan TinggiLiza ApseraBelum ada peringkat
- Pendekatan Lab Pada Short StatureDokumen20 halamanPendekatan Lab Pada Short Staturepdf pediatriBelum ada peringkat
- Diagnosis Perawakan PendekDokumen33 halamanDiagnosis Perawakan PendekRenata YolandaBelum ada peringkat
- Referat Perawakan PendekDokumen19 halamanReferat Perawakan PendekIndahMutiaraBelum ada peringkat
- Gangguan Pertumbuhan PBLDokumen43 halamanGangguan Pertumbuhan PBLYetty M TambunBelum ada peringkat
- Defisiensi Hormon PertumbuhanDokumen19 halamanDefisiensi Hormon PertumbuhanMariaFransischa100% (1)
- Bab IiDokumen23 halamanBab IiKhanif Kinesthesia CahyagamaBelum ada peringkat
- StuntingDokumen17 halamanStuntingyunita sariBelum ada peringkat
- Stunting Vs Short Stature DR FaisalDokumen20 halamanStunting Vs Short Stature DR Faisalari aulia rahman hakimBelum ada peringkat
- G1a120015 - Echapatricia WijayaDokumen10 halamanG1a120015 - Echapatricia WijayaSeptian Akbar WijayaBelum ada peringkat
- Pendeknya AnakDokumen20 halamanPendeknya Anakleonjunchan_66965707Belum ada peringkat
- Referat StuntingDokumen27 halamanReferat StuntingdeyaBelum ada peringkat
- Pubertas TardaDokumen15 halamanPubertas TardaJoshuaRobertoPratamaBelum ada peringkat
- Prediksi UKMPPD 3Dokumen534 halamanPrediksi UKMPPD 3Fatih AbdullahBelum ada peringkat
- Perawakan PendekDokumen0 halamanPerawakan PendekLeliana SalehBelum ada peringkat
- Askep GHDokumen42 halamanAskep GHFitra WahyuBelum ada peringkat
- Hormon Pertumbuhan Growth Hormone GHDokumen20 halamanHormon Pertumbuhan Growth Hormone GHlylasherliaBelum ada peringkat
- Makalah Defisiensi Growth HormoneDokumen20 halamanMakalah Defisiensi Growth HormonebVentisaK100% (2)
- Soal PretestDokumen2 halamanSoal PretestAldy RinaldiBelum ada peringkat
- PERTAMAHAN PENDEKDokumen24 halamanPERTAMAHAN PENDEKTri Utami WahyuningsihBelum ada peringkat
- Gangguan Tumbuh KembangDokumen3 halamanGangguan Tumbuh Kembangyuly_chelseaBelum ada peringkat
- STUNTINGDokumen3 halamanSTUNTINGRima Nur AnnisaBelum ada peringkat
- Pubertas TerlambatDokumen7 halamanPubertas TerlambatMahardika Koes R G100% (1)
- TURNERDokumen24 halamanTURNERZainuddin Surkan HBelum ada peringkat
- Dwarfisme Adalah Suatu Kondisi Kelainan Yang Ditandai Dengan Tinggi Tubuh Yang Pendek Akibat Kelainan Medis Atau GenetisDokumen7 halamanDwarfisme Adalah Suatu Kondisi Kelainan Yang Ditandai Dengan Tinggi Tubuh Yang Pendek Akibat Kelainan Medis Atau GenetisNandaBelum ada peringkat
- PertumbuhanHormonDokumen16 halamanPertumbuhanHormonDesi BasukiBelum ada peringkat
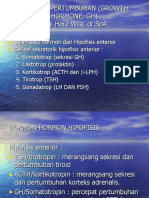
- Hormon Pertumbuhan (Growth Hormone, GH)Dokumen20 halamanHormon Pertumbuhan (Growth Hormone, GH)Rihi Here Wila100% (1)
- Makalah Blok 27 Sindrom TurnerDokumen17 halamanMakalah Blok 27 Sindrom TurnerkrisianBelum ada peringkat
- Jurnal Perawatan Skoliosis Natural Anda: Petunjuk per hari selama 12 minggu untuk tulang belakang yang lebih lurus dan kuat!Dari EverandJurnal Perawatan Skoliosis Natural Anda: Petunjuk per hari selama 12 minggu untuk tulang belakang yang lebih lurus dan kuat!Penilaian: 4.5 dari 5 bintang4.5/5 (7)
- Merawat penyakit kencing manis tanpa ubatDari EverandMerawat penyakit kencing manis tanpa ubatPenilaian: 5 dari 5 bintang5/5 (3)
- Bagaimana cara naik seperti kuda di tempat tidur? Bagaimana menjadi pemain dan pemain yang lebih baik di tempat tidurDari EverandBagaimana cara naik seperti kuda di tempat tidur? Bagaimana menjadi pemain dan pemain yang lebih baik di tempat tidurBelum ada peringkat
- Panduan Esensial untuk Skoliosis dan Kesehatan KehamilanDari EverandPanduan Esensial untuk Skoliosis dan Kesehatan KehamilanPenilaian: 4.5 dari 5 bintang4.5/5 (4)
- BUKU Pedoman Izin Edar Alkes PDFDokumen37 halamanBUKU Pedoman Izin Edar Alkes PDFMita Magnae Avianti75% (4)
- Pedoman Pelayanan Izin Edar Alat Kesehatan BilingualDokumen49 halamanPedoman Pelayanan Izin Edar Alat Kesehatan BilingualkeriBelum ada peringkat
- REGISTRASI ALKES A DAN BDokumen39 halamanREGISTRASI ALKES A DAN BR BunardiBelum ada peringkat
- Prosedur Pengendalian DokumenDokumen6 halamanProsedur Pengendalian DokumenR BunardiBelum ada peringkat
- Distribusi Alkes Yang BaikDokumen18 halamanDistribusi Alkes Yang BaikFajar Agung Prayogo80% (5)
- PP Nomor 32 Tahun 2017Dokumen8 halamanPP Nomor 32 Tahun 2017R BunardiBelum ada peringkat
- Inspeksi Diri (2012)Dokumen31 halamanInspeksi Diri (2012)Rizky Taufik75% (4)
- Bahan Alam Sumber Pendapatan PembangunanDokumen6 halamanBahan Alam Sumber Pendapatan PembangunanR BunardiBelum ada peringkat
- Permenkes 246Dokumen16 halamanPermenkes 246Githa 'gigit' DestrianBelum ada peringkat
- Dokumen Wajib Iso 9001-2015 - SintegralDokumen1 halamanDokumen Wajib Iso 9001-2015 - SintegralR BunardiBelum ada peringkat
- Kajian JamuDokumen265 halamanKajian Jamuariffatul lailatussholikhahBelum ada peringkat
- PeraturanDokumen4 halamanPeraturanR BunardiBelum ada peringkat
- CDA OPerasionalDokumen2 halamanCDA OPerasionalR BunardiBelum ada peringkat
- Kajian JamuDokumen265 halamanKajian Jamuariffatul lailatussholikhahBelum ada peringkat
- Memperkenalkan Akupunktur GI Dalam Upaya Peningkatan Kesehatan MasyarakatDokumen2 halamanMemperkenalkan Akupunktur GI Dalam Upaya Peningkatan Kesehatan MasyarakatR BunardiBelum ada peringkat
- Analisis Data MinitabDokumen4 halamanAnalisis Data MinitabR BunardiBelum ada peringkat
- Akuisisi PerusahaanDokumen22 halamanAkuisisi PerusahaanR BunardiBelum ada peringkat
- Pengawasan Pangan Berlabel Halal1Dokumen42 halamanPengawasan Pangan Berlabel Halal1Nurul FajrinaBelum ada peringkat
- Obat TradisionalDokumen50 halamanObat TradisionalAlzamri FhilzaBelum ada peringkat
- Karakteristik KlorinDokumen7 halamanKarakteristik KlorinUcu KhoerunisaBelum ada peringkat
- Pengawasan Pangan Berlabel Halal1Dokumen42 halamanPengawasan Pangan Berlabel Halal1Nurul FajrinaBelum ada peringkat
- Pedoman Praktik Apoteker Indonesia 2013Dokumen53 halamanPedoman Praktik Apoteker Indonesia 2013Ferdina Recky100% (2)
- Tata UdaraDokumen9 halamanTata UdaraRizkiyahBelum ada peringkat
- HPLCDokumen24 halamanHPLCNierza AlfiannurBelum ada peringkat
- Permenkes 1148 2011 Tentang PBFDokumen19 halamanPermenkes 1148 2011 Tentang PBFTrisna SuksesBelum ada peringkat
- Karakteristik KlorinDokumen7 halamanKarakteristik KlorinUcu KhoerunisaBelum ada peringkat
- AbstrakDokumen11 halamanAbstrakR BunardiBelum ada peringkat
- Tugas Dan Wewenang Apoteker Revisi ManadoDokumen5 halamanTugas Dan Wewenang Apoteker Revisi ManadoSerpentarius_05Belum ada peringkat
- 2006-2-01105-TI-Bab 2Dokumen32 halaman2006-2-01105-TI-Bab 2R BunardiBelum ada peringkat