Anda mungkin juga menyukai
- Canadian Contraception ConsensusDokumen14 halamanCanadian Contraception Consensusjo_jo_maniaBelum ada peringkat
- Donordarah PDFDokumen1 halamanDonordarah PDFjo_jo_maniaBelum ada peringkat
- Case Report: Pulmonary Sequestration: A Case Report and Literature ReviewDokumen4 halamanCase Report: Pulmonary Sequestration: A Case Report and Literature Reviewjo_jo_maniaBelum ada peringkat
- Structure Content: 1. EXERCISE 1 (Skill 1-2) 2. Toefl Review Exercise (Skill 1-2) 3. Answer KeysDokumen3 halamanStructure Content: 1. EXERCISE 1 (Skill 1-2) 2. Toefl Review Exercise (Skill 1-2) 3. Answer Keysjo_jo_mania0% (1)
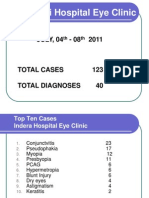
- NEW Weekly Indra 04-08 July 2011Dokumen13 halamanNEW Weekly Indra 04-08 July 2011jo_jo_maniaBelum ada peringkat
- Donor DarahDokumen1 halamanDonor Darahjo_jo_maniaBelum ada peringkat
- AnyelirDokumen2 halamanAnyelirjo_jo_maniaBelum ada peringkat
- Laser Iridotomy and GlaucomaDokumen2 halamanLaser Iridotomy and Glaucomajo_jo_maniaBelum ada peringkat
- International Centre For Eye Health Teaching Set 2 The Eye in Primary Health CareDokumen25 halamanInternational Centre For Eye Health Teaching Set 2 The Eye in Primary Health Carejo_jo_maniaBelum ada peringkat
- OrtoDokumen61 halamanOrtojo_jo_maniaBelum ada peringkat
- Migraine Prophylaxis: Pharmacotherapy PerspectivesDokumen11 halamanMigraine Prophylaxis: Pharmacotherapy Perspectivesjo_jo_maniaBelum ada peringkat
- Sunday, 26/09 /2010 PT/LN/MG:: Consultant DR Mas Putra SPMDokumen6 halamanSunday, 26/09 /2010 PT/LN/MG:: Consultant DR Mas Putra SPMjo_jo_maniaBelum ada peringkat
- Arterial Blood Gas: DR - Made Widia, Sp.A (K)Dokumen19 halamanArterial Blood Gas: DR - Made Widia, Sp.A (K)jo_jo_mania100% (1)
- Histamin Dan inDokumen30 halamanHistamin Dan inNurul FadilaturrahmiBelum ada peringkat
- X RaysDokumen1 halamanX Raysjo_jo_maniaBelum ada peringkat
- Dyslexia: Developmental Dyslexia Is ADokumen5 halamanDyslexia: Developmental Dyslexia Is Ajo_jo_mania100% (1)
- UveaDokumen43 halamanUveajo_jo_mania100% (1)
- An Endometrial Is A Procedure To Remove A Small Sample of The Lining of The UterusDokumen2 halamanAn Endometrial Is A Procedure To Remove A Small Sample of The Lining of The Uterusjo_jo_maniaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Vocabulary Words - 20.11Dokumen2 halamanVocabulary Words - 20.11ravindra kumar AhirwarBelum ada peringkat
- Law - Midterm ExamDokumen2 halamanLaw - Midterm ExamJulian Mernando vlogsBelum ada peringkat
- Sportex 2017Dokumen108 halamanSportex 2017AleksaE77100% (1)
- DB - Empirically Based TheoriesDokumen3 halamanDB - Empirically Based TheoriesKayliah BaskervilleBelum ada peringkat
- Three Categories of AutismDokumen14 halamanThree Categories of Autismapi-327260204Belum ada peringkat
- Prestressed ConcreteDokumen66 halamanPrestressed ConcreteTech BisuBelum ada peringkat
- ANTH 222 Syllabus 2012Dokumen6 halamanANTH 222 Syllabus 2012Maythe S. HanBelum ada peringkat
- Value Chain AnalaysisDokumen100 halamanValue Chain AnalaysisDaguale Melaku AyeleBelum ada peringkat
- Robert FrostDokumen15 halamanRobert FrostRishi JainBelum ada peringkat
- Sultan Omar Ali Saifuddin IIIDokumen14 halamanSultan Omar Ali Saifuddin IIISekolah Menengah Rimba100% (3)
- Signal&Systems - Lab Manual - 2021-1Dokumen121 halamanSignal&Systems - Lab Manual - 2021-1telecom_numl8233Belum ada peringkat
- Cooking Oils and Smoke Points - What To Know and How To Choose The Right Cooking Oil - 2020 - MasterClassDokumen7 halamanCooking Oils and Smoke Points - What To Know and How To Choose The Right Cooking Oil - 2020 - MasterClasschumbefredBelum ada peringkat
- Comparing Effect of Adding LDPE, PP, PMMA On The Mechanical Properties of Polystyrene (PS)Dokumen12 halamanComparing Effect of Adding LDPE, PP, PMMA On The Mechanical Properties of Polystyrene (PS)Jawad K. OleiwiBelum ada peringkat
- 2011 06 13-DI-PER8-Acoustic Insulation Catalogue-Rev 01Dokumen12 halaman2011 06 13-DI-PER8-Acoustic Insulation Catalogue-Rev 01Tien PhamBelum ada peringkat
- Didhard Muduni Mparo and 8 Others Vs The GRN of Namibia and 6 OthersDokumen20 halamanDidhard Muduni Mparo and 8 Others Vs The GRN of Namibia and 6 OthersAndré Le RouxBelum ada peringkat
- Group 1 Reviewer Social LegislationDokumen5 halamanGroup 1 Reviewer Social Legislationxsar_xBelum ada peringkat
- X-Roc Latex: Product DescriptionDokumen2 halamanX-Roc Latex: Product DescriptionAmr RagabBelum ada peringkat
- Civil Engineering Interview QuestionsDokumen19 halamanCivil Engineering Interview QuestionsSrivardhanSrbBelum ada peringkat
- Student Management System - Full DocumentDokumen46 halamanStudent Management System - Full DocumentI NoBelum ada peringkat
- Bakery Management SynopsisDokumen13 halamanBakery Management SynopsisSHiVaM KRBelum ada peringkat
- ReportDokumen8 halamanReportTrust Asia Cargo in OfficeBelum ada peringkat
- Total ChangeDokumen9 halamanTotal ChangeaurennosBelum ada peringkat
- Review of Related LiteratureDokumen9 halamanReview of Related LiteratureMarion Joy GanayoBelum ada peringkat
- Baixar Livro Draw With Jazza Creating Characters de Josiah Broo PDFDokumen5 halamanBaixar Livro Draw With Jazza Creating Characters de Josiah Broo PDFCarlos Mendoza25% (4)
- 5.4 Marketing Arithmetic For Business AnalysisDokumen12 halaman5.4 Marketing Arithmetic For Business AnalysisashBelum ada peringkat
- Forensic BallisticsDokumen23 halamanForensic BallisticsCristiana Jsu DandanBelum ada peringkat
- Not Just Another Winter Festival: Rabbi Reuven BrandDokumen4 halamanNot Just Another Winter Festival: Rabbi Reuven Brandoutdash2Belum ada peringkat
- IN THE BEGINNING WAS AFFECT RolnikDokumen22 halamanIN THE BEGINNING WAS AFFECT RolnikFabiana PaulinoBelum ada peringkat
- The Civil Mutinies of Romeo and Juliet: Glenn ClarkDokumen21 halamanThe Civil Mutinies of Romeo and Juliet: Glenn ClarkmilcahBelum ada peringkat
- Design and Experimental Performance Assessment of An Outer Rotor PM Assisted SynRM For The Electric Bike PropulsionDokumen11 halamanDesign and Experimental Performance Assessment of An Outer Rotor PM Assisted SynRM For The Electric Bike PropulsionTejas PanchalBelum ada peringkat