Anda mungkin juga menyukai
- Icra PpiDokumen4 halamanIcra Ppiyusufharkian186% (28)
- Penilaian Kinerja Perawat (Contoh) PDFDokumen1 halamanPenilaian Kinerja Perawat (Contoh) PDFFitri YahutBelum ada peringkat
- Materi RDKK Kamis 18 Agst 2022Dokumen18 halamanMateri RDKK Kamis 18 Agst 2022mela gustianaBelum ada peringkat
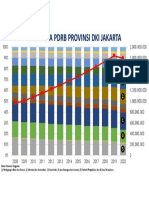
- Dinamika PDRB DKI JakartaDokumen1 halamanDinamika PDRB DKI JakartaBayu WirawanBelum ada peringkat
- Catatan Penggunaan Obat Di Kotak p3kDokumen2 halamanCatatan Penggunaan Obat Di Kotak p3kjimivritBelum ada peringkat
- Lembar Penilaian Juri 23Dokumen1 halamanLembar Penilaian Juri 23shadiq NBelum ada peringkat
- Daftar Program KerjaDokumen6 halamanDaftar Program KerjaPutri AzizahBelum ada peringkat
- Form. 13 Rekapitulasi Rekomendasi Tim VerifikasiDokumen1 halamanForm. 13 Rekapitulasi Rekomendasi Tim Verifikasibumdesma lkdBelum ada peringkat
- Form ProduksiDokumen1 halamanForm ProduksiPriyo SaputroBelum ada peringkat
- 02 Risk Assessment - Penyelesaian PiutangDokumen3 halaman02 Risk Assessment - Penyelesaian PiutangMaintenance ITBelum ada peringkat
- 01 Risk Assessment - Pencatatan Aktiva TetapDokumen3 halaman01 Risk Assessment - Pencatatan Aktiva TetapMaintenance ITBelum ada peringkat
- Rumah Sakit Pku Muhammadiyah Gombong: (Unit Tower)Dokumen1 halamanRumah Sakit Pku Muhammadiyah Gombong: (Unit Tower)buatapa301Belum ada peringkat
- Spo Penyimpanan Darah Di Blood Refrigerator Rev 24 Sept 2022Dokumen5 halamanSpo Penyimpanan Darah Di Blood Refrigerator Rev 24 Sept 2022rakhatiarBelum ada peringkat
- Form ProduksiDokumen3 halamanForm ProduksiPriyo SaputroBelum ada peringkat
- Format Laporan Kondisi UnitDokumen5 halamanFormat Laporan Kondisi UnitArdiBelum ada peringkat
- Lampiran 1-13xDokumen20 halamanLampiran 1-13xItkab OkiBelum ada peringkat
- Pengembangan Sistem Manajemen PNSDokumen2 halamanPengembangan Sistem Manajemen PNSQusnul SyamsudinBelum ada peringkat
- Oppm MoralDokumen12 halamanOppm MoralTJ KutikBelum ada peringkat
- Drawing 2Dokumen1 halamanDrawing 2roy zonthara simbolonBelum ada peringkat
- Rew LAPORAN HARIAN AMBULANCE 2 CHECK LIST PEMAKAIAN AMBULANCE EMERGENCYDokumen1 halamanRew LAPORAN HARIAN AMBULANCE 2 CHECK LIST PEMAKAIAN AMBULANCE EMERGENCYYARSI JAKARTABelum ada peringkat
- Ruk 2024 Poli GigiDokumen14 halamanRuk 2024 Poli GigiAyu Devi YantiBelum ada peringkat
- Cakranhuwana - SiteplanDokumen1 halamanCakranhuwana - SiteplanIlhamBelum ada peringkat
- Kesepakatan Agenda 4Dokumen18 halamanKesepakatan Agenda 4NurulhudaBelum ada peringkat
- Penetapan Prioritas Pengukuran Mutu Dan Penyusunan Kamus IndikatorDokumen13 halamanPenetapan Prioritas Pengukuran Mutu Dan Penyusunan Kamus Indikatorwahyu KurniawanBelum ada peringkat
- Blanko Rawat Jalan Jamkesmas NewDokumen1 halamanBlanko Rawat Jalan Jamkesmas NewDIDIK KARYANTO DIDIK KARYANTOBelum ada peringkat
- Program Pemantauan Dan Pengukuran 2019Dokumen2 halamanProgram Pemantauan Dan Pengukuran 2019Ndi FarhanBelum ada peringkat
- Blanko YankestradDokumen19 halamanBlanko Yankestradjumratul seftrianiBelum ada peringkat
- Daftar Hadir Safety InductionDokumen2 halamanDaftar Hadir Safety InductionSari Dian AnggraeniBelum ada peringkat
- Log Book KeperawatanDokumen14 halamanLog Book KeperawatanTitik ErawatiBelum ada peringkat
- Oppm Panitia Bi 2Dokumen7 halamanOppm Panitia Bi 2kamawisBelum ada peringkat
- Form Blood PressureDokumen1 halamanForm Blood PressureFriska AndaniBelum ada peringkat
- Formulir Ketepatan Pemberian Makan PasienDokumen4 halamanFormulir Ketepatan Pemberian Makan PasienTyas Tri WahyuniBelum ada peringkat
- 1 Jadwal Penugasan Personil-OkDokumen2 halaman1 Jadwal Penugasan Personil-OkStanjho DewyBelum ada peringkat
- 1.6.4 (6) - Borang OPCDokumen1 halaman1.6.4 (6) - Borang OPCZainal HarunBelum ada peringkat
- PJ Unit/Program:: Rencana Usulan Kegiatan (Ruk) TAHUN 2024 Unit/Program: Poli GigiDokumen1 halamanPJ Unit/Program:: Rencana Usulan Kegiatan (Ruk) TAHUN 2024 Unit/Program: Poli GigiGugun GumelarBelum ada peringkat
- Cara Menyusun Program Sesuai Standar AkredDokumen14 halamanCara Menyusun Program Sesuai Standar AkredEva SulitaBelum ada peringkat
- Matriks Usulan Program-Perencaan KeslingDokumen5 halamanMatriks Usulan Program-Perencaan KeslingHeryatiBelum ada peringkat
- Poa DinkesDokumen4 halamanPoa DinkesUrip Kudu SabarBelum ada peringkat
- OPPM Panitia Kesenian Tahun 2020Dokumen3 halamanOPPM Panitia Kesenian Tahun 2020Chekgu HarniniBelum ada peringkat
- Batas Lahan: SiteplanDokumen1 halamanBatas Lahan: Siteplanfrandy wonokBelum ada peringkat
- Ida Lokboog Ahli Muda Jan 24Dokumen4 halamanIda Lokboog Ahli Muda Jan 24denyrahmawatiBelum ada peringkat
- Form Kontrol Pencairan Program Sembako Lombok Timur Tahun 2020Dokumen3 halamanForm Kontrol Pencairan Program Sembako Lombok Timur Tahun 2020Damar WulanBelum ada peringkat
- Asessories Jumlah: Dinas Perumahan Rakyat Dan Kawasan PermukimanDokumen1 halamanAsessories Jumlah: Dinas Perumahan Rakyat Dan Kawasan Permukimanpangky atphBelum ada peringkat
- Check Sheet PreventifDokumen4 halamanCheck Sheet Preventifandriansyahferry1331Belum ada peringkat
- Data STBM Kec Minas Minas 2022Dokumen208 halamanData STBM Kec Minas Minas 2022Al MukhalisBelum ada peringkat
- Laporan Bulanan W2Dokumen1 halamanLaporan Bulanan W2Maya NettaBelum ada peringkat
- Analisis Site Spa 04Dokumen9 halamanAnalisis Site Spa 04Rio TampatyBelum ada peringkat
- FMEADokumen2 halamanFMEADian Razak Bastian100% (1)
- Lampiran 3 RUK-RPKDokumen6 halamanLampiran 3 RUK-RPKHeri KuswantoroBelum ada peringkat
- Lampiran 7 - 9Dokumen5 halamanLampiran 7 - 9Luqman Abdul HakimBelum ada peringkat
- Peta Tahun Tanam Afd BandelDokumen1 halamanPeta Tahun Tanam Afd Bandelgatot iriantoBelum ada peringkat
- Checklis Pemeriksaan GensetDokumen1 halamanChecklis Pemeriksaan GensetSiti DarningsihBelum ada peringkat
- Form Klaim Gaji Cimory P03 2023Dokumen1 halamanForm Klaim Gaji Cimory P03 2023safi uddinBelum ada peringkat
- Lembar Kontrol PelaksanaDokumen2 halamanLembar Kontrol PelaksanaTri SulkhaniBelum ada peringkat
- Oppm ts25 KohortDokumen7 halamanOppm ts25 KohortDAYANG KAMARIAH BT AWANG HIDUP MoeBelum ada peringkat
- Form Absen KTM Desember 2023 - Januari 2024Dokumen1 halamanForm Absen KTM Desember 2023 - Januari 2024Biji DurianBelum ada peringkat
- Format Laporan HarianDokumen2 halamanFormat Laporan HarianDIAN EKA SAPUTRABelum ada peringkat