Anda mungkin juga menyukai
- Vertigo Update New Edit NewDokumen56 halamanVertigo Update New Edit NewekiferdiantoBelum ada peringkat
- Penyuluhan EpilepsiDokumen16 halamanPenyuluhan EpilepsiNaurah Al-HaddadBelum ada peringkat
- Mati Otak - A MawuntuDokumen60 halamanMati Otak - A MawuntuBernie BernardusBelum ada peringkat
- Kurnia Kusumastuti (Cara Pelaporan EEG)Dokumen23 halamanKurnia Kusumastuti (Cara Pelaporan EEG)ernita fitrianiBelum ada peringkat
- Gangguan Medula Spinalis 2Dokumen92 halamanGangguan Medula Spinalis 2wiraBelum ada peringkat
- FT Keswan - Fisioterapi Pada VertigoDokumen50 halamanFT Keswan - Fisioterapi Pada VertigofirmandotindraBelum ada peringkat
- Pemeriksaan Klinis NeurologiDokumen52 halamanPemeriksaan Klinis NeurologithyadinarBelum ada peringkat
- VertigoDokumen71 halamanVertigosweet123 cakeBelum ada peringkat
- f43 Reaction To Severe Stress, and AdjustmentDokumen5 halamanf43 Reaction To Severe Stress, and AdjustmentRizqi Aji ApriliaBelum ada peringkat
- Case Report Paralisis Periodik Ec Hipokalemia BeratDokumen39 halamanCase Report Paralisis Periodik Ec Hipokalemia BeratDewiDwipayantiGiriBelum ada peringkat
- Meningitis Kriptokokus KriptokokusDokumen34 halamanMeningitis Kriptokokus KriptokokusBal IndaBelum ada peringkat
- Kuliah Pemeriksaan NeurologiDokumen109 halamanKuliah Pemeriksaan NeurologiZidni Arifa LuthfiBelum ada peringkat
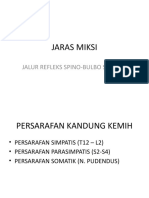
- Jaras MiksiDokumen26 halamanJaras MiksiEvan JSBelum ada peringkat
- Laporan Kasus Tumor CerebriDokumen29 halamanLaporan Kasus Tumor CerebriWahyu AjiBelum ada peringkat
- Kuesioner Untuk Mendiagnosis Nyeri NeuropatikDokumen1 halamanKuesioner Untuk Mendiagnosis Nyeri NeuropatikSatriya PranataBelum ada peringkat
- Referat Sistem LimbikDokumen15 halamanReferat Sistem LimbikEdo Johanes SihombingBelum ada peringkat
- PESERTA - INTERNA 3 - MANTAP Mei 2018 - Unlocked - PDFDokumen200 halamanPESERTA - INTERNA 3 - MANTAP Mei 2018 - Unlocked - PDFFikri UdinBelum ada peringkat
- Sindrom Epilepsi Pada Bayi Dan AnakDokumen20 halamanSindrom Epilepsi Pada Bayi Dan AnakfadhlialbaniBelum ada peringkat
- Pemeriksaan NeurologiDokumen115 halamanPemeriksaan NeurologiAndi Wulandari DjoyosoemartoBelum ada peringkat
- Lobus Temporal (Presentasi)Dokumen9 halamanLobus Temporal (Presentasi)zack zackBelum ada peringkat
- Neuro Oftal KirimDokumen64 halamanNeuro Oftal KirimLiyanti RinceBelum ada peringkat
- Skenario KejangDokumen37 halamanSkenario KejangOlivia DwimaswastiBelum ada peringkat
- Neuropati DiabetikDokumen11 halamanNeuropati DiabetikMuhammad Rizal AdriyansyahBelum ada peringkat
- Juvenile AbsanDokumen2 halamanJuvenile AbsanSlamet PamujiBelum ada peringkat
- MCQ Neuroonkologi 1Dokumen2 halamanMCQ Neuroonkologi 1Kristiana MargaretaBelum ada peringkat
- Tata Cara Pemeriksaan NeurologiDokumen60 halamanTata Cara Pemeriksaan NeurologiBill Brenton Raynherzh MandalaBelum ada peringkat
- Patofisiologi EpilepsiDokumen11 halamanPatofisiologi EpilepsiSeptiani KusumaningtyasBelum ada peringkat
- Simpo 10 Gangguan Metabolik Related Neurologi - Dr. Agus Soedomo, SP.S (K) - RestlessLegs Syndrome Update in Diagnosis and ManagementDokumen52 halamanSimpo 10 Gangguan Metabolik Related Neurologi - Dr. Agus Soedomo, SP.S (K) - RestlessLegs Syndrome Update in Diagnosis and ManagementfairuzBelum ada peringkat
- Neurotrauma Emergency - Yetty RamliDokumen40 halamanNeurotrauma Emergency - Yetty RamliMonica Damayani SusiloBelum ada peringkat
- Insomnia PsqiDokumen23 halamanInsomnia PsqiSofiaRhosmaBelum ada peringkat
- Hubungan Terapi Hiperbarik Oksigen Terhadap StrokeDokumen19 halamanHubungan Terapi Hiperbarik Oksigen Terhadap StrokeEndhiitaBelum ada peringkat
- Langkah-Langkah DiagnosisDokumen14 halamanLangkah-Langkah DiagnosiscipaBelum ada peringkat
- Referat Adem Alhamdulilah FixDokumen33 halamanReferat Adem Alhamdulilah FixayubahriBelum ada peringkat
- Case SNNTDokumen21 halamanCase SNNTAnnyKusumadewiAkbarBelum ada peringkat
- PENYULUHAN Parkinson Edit PDFDokumen15 halamanPENYULUHAN Parkinson Edit PDFAb RamadhanBelum ada peringkat
- Pengertian EpilepsiDokumen6 halamanPengertian Epilepsisaryati kesmasBelum ada peringkat
- Penyakit Moyamoya Dan Sindrom MoyamoyaDokumen19 halamanPenyakit Moyamoya Dan Sindrom MoyamoyaTri Kartika UtomoBelum ada peringkat
- Case Report Anak Nella AFP - Gizi Buruk PPDokumen66 halamanCase Report Anak Nella AFP - Gizi Buruk PPnellanjelBelum ada peringkat
- Keseimbangan Cairan & ElektrolitDokumen49 halamanKeseimbangan Cairan & Elektroliticcha buntoroBelum ada peringkat
- Webinar GeriatriDokumen30 halamanWebinar Geriatriika100% (1)
- Pasien Dengan Gerstmann SyndromeDokumen13 halamanPasien Dengan Gerstmann SyndromeNovi Yanti NyBelum ada peringkat
- VertigoDokumen11 halamanVertigoodiliamariacattleyaBelum ada peringkat
- Mini ProjectDokumen54 halamanMini ProjectSarah Stevany MundaBelum ada peringkat
- EWSS in Patient's Neurologic Winda FIXDokumen53 halamanEWSS in Patient's Neurologic Winda FIXReymon Sihombing100% (1)
- Lapkas Adenoma HipofisisDokumen34 halamanLapkas Adenoma HipofisispocutindahBelum ada peringkat
- Hernia Nukleus Pulposus (HNP)Dokumen20 halamanHernia Nukleus Pulposus (HNP)ami diyBelum ada peringkat
- Kesadaran MenurunDokumen69 halamanKesadaran Menurunmiftahul jannahBelum ada peringkat
- TiaDokumen12 halamanTiadidit_fajar_N100% (2)
- Low Back PainDokumen106 halamanLow Back PainchetrisriBelum ada peringkat
- Referat Kejang LiaDokumen32 halamanReferat Kejang LiaScribdMeUpBelum ada peringkat
- Buku Pedoman SPM PDFDokumen197 halamanBuku Pedoman SPM PDFhesstyBelum ada peringkat
- Nyeri NeuropatikDokumen8 halamanNyeri NeuropatikfaridahakimlBelum ada peringkat
- Pemeriksaan Status Mental Strub Dan Black Versi IndonesiaDokumen1 halamanPemeriksaan Status Mental Strub Dan Black Versi IndonesiaNastiti WidyariniBelum ada peringkat
- Diagnosis Dan Penatalaksanaan Tuli MendadakDokumen36 halamanDiagnosis Dan Penatalaksanaan Tuli MendadakAlvin WayanBelum ada peringkat
- Gangguan GerakDokumen48 halamanGangguan GerakNelli Nur Indah SariBelum ada peringkat
- SKENARIO 1 Modul Kel 11 Musculoskeletal FixDokumen38 halamanSKENARIO 1 Modul Kel 11 Musculoskeletal FixAsbar Fatur MuhBelum ada peringkat
- Penyakit ParkinsonDokumen13 halamanPenyakit ParkinsonRichella Khansa LaudittaBelum ada peringkat
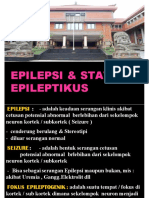
- Epilepsi Dan Status Epileptikus PDFDokumen57 halamanEpilepsi Dan Status Epileptikus PDFOdi BayuBelum ada peringkat
- Support Slide Responsi EpilepsiDokumen52 halamanSupport Slide Responsi EpilepsiNindhyaPutriBelum ada peringkat
- Tentiran EpilepsiDokumen59 halamanTentiran EpilepsiYuniarHisaPratiwiSuronoBelum ada peringkat
- 9.4.2.1 Laporan Hasil Monitoring Mutu Layanan KlinisDokumen5 halaman9.4.2.1 Laporan Hasil Monitoring Mutu Layanan KlinisRestu Iswara100% (5)
- Kerangka Acuan Kegiatan Pelatihan AparDokumen4 halamanKerangka Acuan Kegiatan Pelatihan AparRoma Fahriza100% (2)
- Sop Rujukan Rawat JLNDokumen4 halamanSop Rujukan Rawat JLNariesBelum ada peringkat
- 9.4.2.1 Laporan Hasil Monitoring Mutu Layanan Klinis Dan Keselamatan PasienDokumen2 halaman9.4.2.1 Laporan Hasil Monitoring Mutu Layanan Klinis Dan Keselamatan PasienYoan Bupati100% (1)
- 9 4 2 6 SK Penanggung Jawab Pelaksanaan Kegiatan PerbaikanDokumen3 halaman9 4 2 6 SK Penanggung Jawab Pelaksanaan Kegiatan PerbaikanYasmin AlqadriBelum ada peringkat
- 9.4.2.1 Laporan Hasil Monitoring Mutu Layanan Klinis Dan Keselamatan PasienDokumen2 halaman9.4.2.1 Laporan Hasil Monitoring Mutu Layanan Klinis Dan Keselamatan PasienYoan Bupati100% (1)
- 9.4.2.1 Laporan Hasil Monitoring Mutu Layanan Klinis Dan Keselamatan PasienDokumen2 halaman9.4.2.1 Laporan Hasil Monitoring Mutu Layanan Klinis Dan Keselamatan PasienYoan Bupati100% (1)
- 9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan PasienDokumen4 halaman9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan Pasienical100% (2)
- SOP Survey Kepuasan PasienDokumen2 halamanSOP Survey Kepuasan PasienEvaBelum ada peringkat
- 7 5 4 B Persyaratan Kompetensi Petugas Yang Melakukan Monitoring Dan Bukti PelaksanaanyaDokumen3 halaman7 5 4 B Persyaratan Kompetensi Petugas Yang Melakukan Monitoring Dan Bukti PelaksanaanyaYasmin AlqadriBelum ada peringkat
- Sop Perdarahan AntepartumDokumen4 halamanSop Perdarahan AntepartumEly Utary60% (10)
- Alur Kamar BersalinDokumen3 halamanAlur Kamar BersalinIlham Akbar75% (4)
- 7 1 3 Ep 4 Persyaratan Kompetensi Petugas Pola Ketenagaan Dan Kesesuaian Terhadap Persyaratan Kompetensi Dan Pola Ketenagaan Pelatihan Yang DiikutiDokumen1 halaman7 1 3 Ep 4 Persyaratan Kompetensi Petugas Pola Ketenagaan Dan Kesesuaian Terhadap Persyaratan Kompetensi Dan Pola Ketenagaan Pelatihan Yang DiikutiYasmin AlqadriBelum ada peringkat
- 9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan PasienDokumen4 halaman9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan Pasienical100% (2)
- Alur Kamar BersalinDokumen3 halamanAlur Kamar BersalinIlham Akbar75% (4)
- 9.2.2 Sop Pelayanan KlinisDokumen3 halaman9.2.2 Sop Pelayanan Klinisdokter irman67% (6)
- 9.4.1.a SK Tenaga Klinis Yang Terlibat Upaya Peningkatan MutuDokumen3 halaman9.4.1.a SK Tenaga Klinis Yang Terlibat Upaya Peningkatan Mutuical100% (3)
- 9.4.1.a SK Tenaga Klinis Yang Terlibat Upaya Peningkatan MutuDokumen3 halaman9.4.1.a SK Tenaga Klinis Yang Terlibat Upaya Peningkatan Mutuical100% (3)
- 9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan PasienDokumen4 halaman9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan Pasienical100% (2)
- SOP Survey Kepuasan PasienDokumen2 halamanSOP Survey Kepuasan PasienEvaBelum ada peringkat
- Alur Kamar BersalinDokumen3 halamanAlur Kamar BersalinIlham Akbar75% (4)
- 9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan PasienDokumen4 halaman9.4.1.b SK Pembentukan Tim Peningkatan Mutu Dan Keselamatan Pasienical100% (2)
- SOP Survey Kepuasan PasienDokumen2 halamanSOP Survey Kepuasan PasienEvaBelum ada peringkat
- Kerangka Acuan PMKPDokumen4 halamanKerangka Acuan PMKPVirgie Fabian100% (1)
- Kerangka Acuan PMKPDokumen4 halamanKerangka Acuan PMKPVirgie Fabian100% (1)
- Daftar Tilik Pendaftaran Pasien Bab VIIDokumen3 halamanDaftar Tilik Pendaftaran Pasien Bab VIIRina ElisaBelum ada peringkat
- Daftar Tilik SopDokumen22 halamanDaftar Tilik Sopsunarni100% (4)
- Indikator SPM UKP PuskesmasDokumen37 halamanIndikator SPM UKP PuskesmasYoga Wicaksana100% (2)
- Daftar Tilik SopDokumen22 halamanDaftar Tilik Sopsunarni100% (4)
- Emergen Si in Dental PracticeDokumen29 halamanEmergen Si in Dental PracticeDwi ZirobeBelum ada peringkat