Anda mungkin juga menyukai
- Program-Kerja MPPDokumen3 halamanProgram-Kerja MPPAnonymous ZzTqbf8100% (9)
- Panduan Case Manager-MppDokumen13 halamanPanduan Case Manager-Mppyessica sallyvania88% (8)
- Pp. 2 Panduan Case Manajer PDFDokumen12 halamanPp. 2 Panduan Case Manajer PDFArif Riyanto83% (6)
- SPO Pengisian Form MPPDokumen4 halamanSPO Pengisian Form MPPNhaoci Oci100% (5)
- Buku Panduan Praktik Manajer Pelayanan Pasien (MPP) - Edisi II, Juli 2016Dokumen40 halamanBuku Panduan Praktik Manajer Pelayanan Pasien (MPP) - Edisi II, Juli 2016Ifang Gunawan100% (20)
- Contoh Kasus MPPDokumen5 halamanContoh Kasus MPPAgus Nugraha100% (4)
- Laporan MPPDokumen12 halamanLaporan MPPAndrew Sebastian100% (1)
- Skrining MPP OkDokumen1 halamanSkrining MPP OkEKA100% (1)
- Buku DPJP Oke Mei 15 PDFDokumen49 halamanBuku DPJP Oke Mei 15 PDFnurhayati100% (2)
- Spo Manajemen Pelayanan Pasien (MPP)Dokumen4 halamanSpo Manajemen Pelayanan Pasien (MPP)DITA YUSNI MAISYAROHBelum ada peringkat
- Laporan MPPDokumen17 halamanLaporan MPPmega discha100% (1)
- Draft Panduan Pelaksanaan Case ManagerDokumen7 halamanDraft Panduan Pelaksanaan Case Managertri50480% (5)
- Sosialisasi Case ManagerDokumen35 halamanSosialisasi Case ManagerAndi Tatat100% (5)
- 2 Asuhan Pasien TerintegrasiDokumen26 halaman2 Asuhan Pasien TerintegrasiYuda AristoBelum ada peringkat
- Aplikasi E-Blud PuskesmasDokumen35 halamanAplikasi E-Blud PuskesmasDaniel Cain100% (3)
- Program Kerja Bidang Penelitian & Sistem Informasi KomunikasiDokumen8 halamanProgram Kerja Bidang Penelitian & Sistem Informasi KomunikasiDaniel Cain100% (2)
- Tatalaksana MPPDokumen66 halamanTatalaksana MPPnazvianatasiaBelum ada peringkat
- Peran Dan Fungsi MPPDokumen67 halamanPeran Dan Fungsi MPPDaniel Cain100% (3)
- LPJ Manager CaseDokumen5 halamanLPJ Manager CasesaluhudinBelum ada peringkat
- SPO Skrining MPPDokumen3 halamanSPO Skrining MPPaprilia lutfiyani100% (1)
- Program Kerja Manajer Pelayanan PasienDokumen3 halamanProgram Kerja Manajer Pelayanan PasienOktaviani LamapahaBelum ada peringkat
- Laporan Manager Pelayanan Pasien Bulan Februari 2020..dini AprilianiDokumen5 halamanLaporan Manager Pelayanan Pasien Bulan Februari 2020..dini Aprilianidini aprilianiBelum ada peringkat
- Panduan Pelaksanaan Case Manager 2Dokumen10 halamanPanduan Pelaksanaan Case Manager 2Ipah Maniez100% (2)
- Presentasi Kasus MPPDokumen3 halamanPresentasi Kasus MPPRinni AndrianzzBelum ada peringkat
- SK MPPDokumen10 halamanSK MPPAnnieBelum ada peringkat
- Uraian Tugas MPPDokumen3 halamanUraian Tugas MPPQiew IkiBelum ada peringkat
- Laporan MPPDokumen14 halamanLaporan MPPAndrew Sebastian100% (2)
- SK Pedoman Case - ManagerDokumen4 halamanSK Pedoman Case - ManagerridwanteBelum ada peringkat
- Kebijakan Case ManagerDokumen8 halamanKebijakan Case ManagerIrawan100% (1)
- Fungsi MPPDokumen86 halamanFungsi MPPBELABelum ada peringkat
- Kriteria MPP Discharge PlanningDokumen1 halamanKriteria MPP Discharge Planningadriany100% (2)
- Lembar Kerja Form B - MPPDokumen2 halamanLembar Kerja Form B - MPPMUSARONGAHBelum ada peringkat
- Lembar Latihan Form A - MPP Ekky RS Citra HusadaDokumen3 halamanLembar Latihan Form A - MPP Ekky RS Citra Husadak3 rschBelum ada peringkat
- Penggunaan Form A Dan Form B Rs Kariadi SemarangDokumen40 halamanPenggunaan Form A Dan Form B Rs Kariadi SemarangAmel100% (1)
- Laporan Kegiatan Workshop Case ManagerDokumen20 halamanLaporan Kegiatan Workshop Case ManagerWeny YuarsihBelum ada peringkat
- Contoh Pengisian Form B ImplementasiDokumen2 halamanContoh Pengisian Form B ImplementasigatotawBelum ada peringkat
- Formulir Identifikasi Skrining Pasien MPPDokumen1 halamanFormulir Identifikasi Skrining Pasien MPPlia dianaBelum ada peringkat
- Laporan Kerja MPP Tr1 2021Dokumen10 halamanLaporan Kerja MPP Tr1 2021Eka Supiyandir Ummu HaidarBelum ada peringkat
- Spo MPPDokumen2 halamanSpo MPPfiharjatinBelum ada peringkat
- Lembar Latihan Form A - MPP - MyzardDokumen3 halamanLembar Latihan Form A - MPP - MyzardMyzard AriefBelum ada peringkat
- Spo MPP 1Dokumen2 halamanSpo MPP 1Anonymous s2jVggb85100% (1)
- Panduan MPP 2022Dokumen12 halamanPanduan MPP 2022kalila100% (1)
- Proker MPPDokumen9 halamanProker MPPauliya100% (1)
- ARK-PANDUAN MPP-printDokumen19 halamanARK-PANDUAN MPP-printDanie Ayu FebrianaBelum ada peringkat
- Pedoman MPPDokumen6 halamanPedoman MPPminarni100% (3)
- Panduan MPPDokumen11 halamanPanduan MPPAzhari100% (1)
- SPO Pengisian Formulir A - MPPDokumen2 halamanSPO Pengisian Formulir A - MPPWiwit Andriyani100% (2)
- Case Manager Profesi Baru Di Rumah Sakit IndonesiaDokumen3 halamanCase Manager Profesi Baru Di Rumah Sakit IndonesiaRobertus Arian100% (2)
- Panduan Case ManagerDokumen16 halamanPanduan Case Managerchristian100% (1)
- 06 Panduan Manajer Pelayanan Pasien (Case Manager) Rs Estomihi CetakDokumen8 halaman06 Panduan Manajer Pelayanan Pasien (Case Manager) Rs Estomihi CetakarihBelum ada peringkat
- MPPDokumen79 halamanMPPRatna fatimahBelum ada peringkat
- Drnico Dokumentasi MPP-Okt-2019Dokumen81 halamanDrnico Dokumentasi MPP-Okt-2019Komite KeperawatanBelum ada peringkat
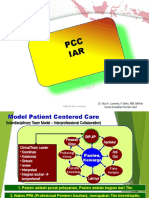
- Slide PCC Iar 08 2014Dokumen13 halamanSlide PCC Iar 08 2014Yopa JariyansyahBelum ada peringkat
- PANDUAN MPP NEW Ok PrintDokumen12 halamanPANDUAN MPP NEW Ok PrintRini AstutiBelum ada peringkat
- 3 DrNico Kolaborasi Interprofesional Mei2015Dokumen34 halaman3 DrNico Kolaborasi Interprofesional Mei2015Suryadi Sarminson100% (2)
- Interkolaborasi PelayananDokumen31 halamanInterkolaborasi PelayananDudang Erawan SusenoBelum ada peringkat
- Presentasi Case Manager Rsud UrmDokumen25 halamanPresentasi Case Manager Rsud Urmjenny100% (1)
- PERAN PPA GIZI Sesuai SNARSDokumen30 halamanPERAN PPA GIZI Sesuai SNARSRina Eka FitrianiBelum ada peringkat
- Panduan MPP-Case MGRDokumen12 halamanPanduan MPP-Case MGRasep saepudinBelum ada peringkat
- Presentasi MPPDokumen10 halamanPresentasi MPPrenny tanoufBelum ada peringkat
- p9 Peran Case ManagerDokumen57 halamanp9 Peran Case ManagerRSGSMBelum ada peringkat
- CPPT Komunikasi EfektifDokumen19 halamanCPPT Komunikasi EfektifFebrianthie ResthyBelum ada peringkat
- Ini Beda Gratifikasi, Suap, Pemerasan, Dan Uang Pelicin - ACLC KPKDokumen4 halamanIni Beda Gratifikasi, Suap, Pemerasan, Dan Uang Pelicin - ACLC KPKDaniel Cain100% (1)
- Belajar Dari Tiga Negara Paling Antikorupsi Di Dunia - ACLC KPKDokumen5 halamanBelajar Dari Tiga Negara Paling Antikorupsi Di Dunia - ACLC KPKDaniel CainBelum ada peringkat
- Memahami 9 Nilai Integritas Untuk Mencegah Korupsi - ACLC KPKDokumen5 halamanMemahami 9 Nilai Integritas Untuk Mencegah Korupsi - ACLC KPKDaniel CainBelum ada peringkat
- Peraturan Internal Staf Keperawatan RSDokumen19 halamanPeraturan Internal Staf Keperawatan RSDaniel CainBelum ada peringkat
- Rev - Persiapan Dokumen OBRA Kabko - Puskesmas - Provinsi Jawa Barat - KABCIREBONDokumen30 halamanRev - Persiapan Dokumen OBRA Kabko - Puskesmas - Provinsi Jawa Barat - KABCIREBONDaniel CainBelum ada peringkat
- Pelaksanaan Vaksinasi Covid-19 Anak - Sign - SignDokumen14 halamanPelaksanaan Vaksinasi Covid-19 Anak - Sign - SignDaniel CainBelum ada peringkat
- Proposal sponsorship-PTMSI RevisiDokumen8 halamanProposal sponsorship-PTMSI RevisiDaniel CainBelum ada peringkat
- Kebijakan TATA KELOLA MUTU DI FKTP, Edit Taufiq 26 Okt 2020Dokumen25 halamanKebijakan TATA KELOLA MUTU DI FKTP, Edit Taufiq 26 Okt 2020Daniel CainBelum ada peringkat
- Materi PendampinganDokumen34 halamanMateri PendampinganDaniel CainBelum ada peringkat
- SK Panita Muscab PtmsiDokumen3 halamanSK Panita Muscab PtmsiDaniel Cain100% (2)
- Budaya Organisasi IslamDokumen14 halamanBudaya Organisasi IslamDaniel CainBelum ada peringkat
- Teknik Melatih - HPHDokumen55 halamanTeknik Melatih - HPHDaniel CainBelum ada peringkat
- Penerapan Managemen Askep Pada Perkesmas Di PuskesmasDokumen84 halamanPenerapan Managemen Askep Pada Perkesmas Di PuskesmasDaniel CainBelum ada peringkat
- Komunikasi EfektifDokumen29 halamanKomunikasi EfektifDaniel CainBelum ada peringkat