Pocket Guide ICT - Edition
Pocket Guide ICT - Edition
Diunggah oleh
Tppi RadiantJudul Asli
Hak Cipta
Format Tersedia
Bagikan dokumen Ini
Apakah menurut Anda dokumen ini bermanfaat?
Apakah konten ini tidak pantas?
Laporkan Dokumen IniHak Cipta:
Format Tersedia
Pocket Guide ICT - Edition
Pocket Guide ICT - Edition
Diunggah oleh
Tppi RadiantHak Cipta:
Format Tersedia
TINJAUAN PUSTAKA
antigen virus yang mirip antigen trombosit, penelitian menyebutkan bahwa rasa lelah membutuhkan terapi walaupun tanpa
disebut juga molecular mimicry, yang kemudian dapat dipengaruhi oleh meningkatnya sitokin perdarahan mukosa.1,4
meningkatkan autoantibodi antiplatelet.7 inflamasi seperti IL-2 dan IFN-Ύ.2
Gangguan autoimun dan limfoproliferatif Angka morbiditas dan mortalitas pasien
juga dapat mendasari terjadinya ITP seperti Pasien ITP memiliki risiko tromboemboli dewasa meningkat sehingga membutuhkan
systemic lupus erythematosus (SLE) dan disebabkan peningkatan antiphospholipid tatalaksana yang lebih kompleks dibandingkan
leukemia limfositik kronis.5 antibodies (APLA).2 pasien anak. Hal ini karena banyak pasien ITP
dewasa berkembang menjadi kasus kronis
DIAGNOSIS dan risiko perdarahan menjadi lebih besar.2,4
Diagnosis melalui beberapa pemeriksaan
dasar seperti anamnesis, pemeriksaan fisik, Target trombosit agar mencapai kondisi
pemeriksaan darah tepi, dan pemeriksaan hemostatik adalah 20-30x109/L.2 Apabila
sumsum tulang belakang. Anamnesis untuk jumlah trombosit di atas 50x109 /L, terapi tidak
riwayat keluarga, riwayat perdarahan, riwayat lagi diperlukan.
penyakit sebelumnya, serta penggunaan obat-
obatan. Pemeriksaan fisik lengkap terutama Pada ITP sekunder yang disebabkan
pada bagian-bagian tubuh yang sering infeksi HCV, eliminasi infeksi dengan obat
mengalami perdarahan seperti mukokutan antivirus dapat meningkatkan trombosit
dan persendian; namun pada sebagian dan menurunkan kadar titer autoantibodi,7
besar pasien ITP tidak didapati kelainan pada namun interferon juga dapat menyebabkan
pemeriksaan fisik.5,9 Pada pasien ITP juga perlu trombositopenia. Apabila terjadi perdarahan,
dicari adanya limfadenopati atau splenomegali IVIg dapat menjadi lini pertama.1 Pada ITP
untuk menyingkirkan keganasan seperti sekunder yang berhubungan dengan HIV,
gangguan limfoproliferatif.5 Pada pasien terapi antiviral dapat langsung diberikan;
dewasa perlu dilakukan pemeriksaan HCV dan terapi ITP jika diperlukan adalah IVIg,
HIV untuk menyingkirkan kemungkinan ITP kortikosteroid, dan anti-D imunoglobulin.1
sekunder.1 Apabila penyebab ITP adalah H.pylori, dapat
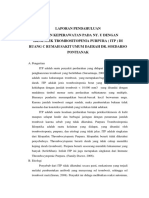
Gambar. Mekanisme terjadinya ITP primer7,8 dilakukan eradikasi H.pylori.7
A. Sel T diaktivasi saat pengenalan antigen oleh Pemeriksaan laboratorium apusan darah
APC menyebabkan aktivasi sel B. Sel B kemudian
memproduksi autoantibodi yang spesifik untuk
tepi merupakan pemeriksaan sederhana Pada ITP primer, terapi lini pertama terdiri dari
glikoprotein trombosit dan megakariosit. yang sangat penting. ITP ditandai dengan kortikosteroid, IVIg, dan IV anti-D, sedangkan
B. Trombosit yang telah berikatan dengan menurunnya jumlah trombosit terisolasi terapi lini kedua terdiri dari splenektomi dan
autoantibodi kemudian berikatan dengan reseptor kurang dari 100.000/µL.1 Trombositopenia tindakan medis lain.2
Fc dan terjadi proses fagositosis pada limpa. terisolasi didefinisikan sebagai
C. Autoantibodi juga berikatan dengan megakariosit trombositopenia tanpa gangguan morfologi Terapi Lini Pertama
sehingga maturasi megakariosit terhambat dan
serta jumlah eritrosit dan leukosit.2,9 Kortikosteroid oral menjadi pilihan utama
juga terjadi destruksi megakariosit
karena efek samping tidak parah, dan tidak
Menurut American Society of Hematology, membutuhkan infus intravena;4 terdiri dari dua
KLINIS pemeriksaan sumsum tulang belakang tidak regimen, yaitu prednison dan deksametason.
Perdarahan merupakan manifestasi klinis perlu karena pemeriksaan apusan darah
yang paling sering. Perdarahan dapat terjadi tepi yang cermat sudah dapat menegakkan Terapi prednison standar dengan dosis 1-2
pada mukokutaneus seperti rongga mulut diagnosis ITP.1 Pada pemeriksaan sumsum mg/kgBB/hari, diberikan hingga terlihat
dan kulit. Perdarahan kulit dapat berupa tulang belakang, dapat ditemukan jumlah respons, kemudian dosis dapat diturunkan
purpura tanpa penyebab yang jelas, pada megakariosit meningkat atau normal, dapat (tapered off).4,5 Deksametason diberikan per
mukosa dapat berupa mimisan, gusi berdarah, terjadi peningkatan jumlah megakariosit oral 40 mg/hari selama 4 hari berturut-turut
dan perdarahan saluran gastrointestinal.2 imatur.2 dan dapat diulang hingga 3 siklus; dosis
Perdarahan intrakranial dan saluran cerna tersebut adalah dosis tinggi. Pada penelitian
sangat jarang namun sangat berbahaya. TATALAKSANA Wei Y, et al, pengobatan ITP dewasa yang baru
Perdarahan intrakranial memiliki insidens Pasien anak yang baru didiagnosis ITP terdiagnosis lebih menguntungkan dengan
kurang dari 0,2% dan terjadi pada jumlah dan tidak memiliki gejala perdarahan atau deksametason dosis tinggi dibandingkan
trombosit kurang dari 10.000/µL.2,3 perdarahan ringan (misalnya perdarahan dengan prednison.10 Pada penelitian
kulit) tidak membutuhkan terapi spesifik dan tersebut, keuntungan yang didapat adalah
Keluhan lain yang sering diabaikan adalah disarankan istirahat total (bed rest).1,4 berkurangnya gejala perdarahan terutama
kelelahan (fatigue). Gejala ini bisa terjadi pada pada stadium awal ITP dan dosis tinggi
pasien ITP dengan trombosit di bawah 10.000/ Pasien dewasa yang baru terdiagnosis ITP deksametason setara dengan pemberian
µL, perdarahan, serta terapi steroid. Beberapa dengan jumlah trombosit di bawah 30x109/L prednison konvensional sehingga dapat
CDK-280/ vol. 46 no. 11 th. 2019 659
PO CKET G U I D E
ASH CLINICAL PRACTICE GUIDELINES
IMMUNE THROMBOCYTOPENIA (ITP)
Management
of Immune
Thrombocytopenia
(ITP)
A POCKET GUIDE FOR THE CLINICIAN
NOVEMBER 2019
Cindy Neunert, MD, Columbia University Medical Center
Sara K. Vesely, PhD, University of Oklahoma Health Sciences Center
Siraj Mithoowani, MD, McMaster University
Taylor Kim, MD, Baylor College of Medicine
The recommendations in this guide are based on the American Society of
Hematology 2019 Guideline for Immune Thrombocytopenia
Context TREATMENT
Immune Thrombocytopenia (ITP) is an acquired autoimmune disorder First-Line Therapies for Adults
characterized by a low platelet count resulting from platelet destruction and
In adults with newly diagnosed ITP, the ASH guideline panel recommends
impaired platelet production. The incidence of ITP is estimated to be 2 to
against a prolonged course (>6 weeks) of prednisone in favor of a
5 per 100,000 persons in the general population and can be an isolated
short course (≤6 weeks) and suggests either prednisone (0.5 - 2.0
primary condition or it may be secondary to other conditions. The information
mg/kg/day) or dexamethasone (40 mg/day for 4 days) as the type of
in this pocket guide is intended to support patients, clinicians, and other
corticosteroid for initial therapy1 . The ASH guideline panel suggests
health professionals in making evidence-based decisions about first-and
corticosteroids alone rather than rituximab and corticosteroids for initial
second-line management of adults and children with ITP.
therapy2 .
1
If a high value is placed on rapidity of platelet count response, an initial course of dexamethasone may be pre-
Adult ferred over prednisone, given that dexamethasone increases the likelihood of a platelet count response at 7 days.
2
If high value is placed on possibility for remission over concerns for potential side effects of rituximab, then an
INPATIENT VS. OUTPATIENT MANAGEMENT initial course of corticosteroids with rituximab may be preferred.
Table 1 – Inpatient vs. Outpatient Management
Good Practice Statement
Platelet Count Status Management For patients receiving corticosteroids, the treating physician should ensure
Platelet count of <20 x109/l Newly diagnosed Inpatient the patient is adequately monitored for potential side effects regardless of the
and asymptomatic or minor duration or type of corticosteroid selected. This includes close monitoring for
mucocutaneous bleeding Established diagnosis Outpatient1 hypertension, hyperglycemia, sleep and mood disturbances, gastric irritation
or ulcer formation, glaucoma, myopathy and osteoporosis. Given the potential
Platelet count of ≥20 x109/l Newly diagnosed Outpatient1 impact of corticosteroids on mental health, the treating physician should
and asymptomatic or minor conduct an assessment of health-related quality of life (HRQoL) (depression,
mucocutaneous bleeding Established diagnosis Outpatient1 fatigue, mental status etc.) while patients are receiving corticosteroids.
1
Patients who are refractory to treatment, those with social concerns, uncertainty about the diagnosis, significant
comorbidities with risk of bleeding, and more significant mucosal bleeding may benefit from admission to the hospital. Second-Line Therapies for Adults
The need for admission is also variable across the range of platelet counts represented here (0-20 x109/l).
In adults with ITP lasting ≥3 months who are corticosteroid-dependent or
Good Practice Statement have no response to corticosteroids, the ASH guideline panel suggests
the following as potential second-line therapies (see Figure 1):
Patients not admitted to the hospital should receive education and expedited
follow-up with a hematologist within 24-72 hours. • Thrombopoietin receptor agonist (eltrombopag or romiplostim)1
• Rituximab
OBSERVATION VS. TREATMENT • Splenectomy2
Determining whether a patient with newly diagnosed ITP should be Follow the algorithm in Figure 1 to determine the most suitable second-
observed or requires pharmacological treatment depends on the degree of line therapies based on presentation and patient preferences.
thrombocytopenia, patient comorbidities, medications, and age – all of which 1
Individual patient preference may place a higher value on the use of a daily oral medication (eltrombopag) or one
impact the risk of bleeding. Management approaches vary based on disease that requires weekly subcutaneous injections (romiplostim).
duration, access to care, quality-of-life implications, and patient and provider 2
If possible, splenectomy should be delayed for at least one year after diagnosis because of the potential for
spontaneous remission in the first year.
preferences, among other factors.
Table 2 - Observation vs. Treatment (Newly Diagnosed ITP) Good Practice Statement
The treating physician should ensure that patients have appropriate
immunizations prior to splenectomy and that they receive counseling regarding
Platelet count ≥30 x 109/l and
asymptomatic or minor mucocutaneous Management with observation1 antibiotic prophylaxis following splenectomy. The treating physician should also
bleeding educate the patient on prompt recognition and management of fever and refer
to current recommendations on pre- and post-splenectomy care.
Platelet count <30 x 109/l and
asymptomatic or minor mucocutaneous Treatment with corticosteroids2 Each of the these second-line treatments may be effective therapy and
bleeding
therefore the choice of treatment should be individualized based on
1
For patients with a platelet count at the lower end of this threshold, for those with additional comorbidities, antico-
duration of ITP, frequency of bleeding episodes requiring hospitalization
agulant or antiplatelet medications, or upcoming procedures, and for elderly patients (>60 years old), treatment with or rescue medication, comorbidities, adherence, medical and social
corticosteroids may be appropriate. support networks, patient values and preferences, cost, and availability.
2
This should include consideration of the severity of thrombocytopenia, additional comorbidities, use of anticoagulant
or antiplatelet medications, need for upcoming procedures, and age of the patient. For example, patients who place a high value on achieving a durable
response may prefer splenectomy or thrombopoietin receptor agonists
(TPO-RAs), patients who value avoidance of long-term medication may
prefer splenectomy or rituximab, and patients who wish to avoid surgery
may prefer a TPO-RA or rituximab. Patient education and shared decision-
making are encouraged.
TINJAUAN PUSTAKA
7. Zufferey A, Kapur R, Semple JW. Pathogenesis and therapeutic mechanisms in immune thrombocytopenia (ITP). J Clin Med. 2017;6(2). pii: E16. doi: 10.3390/
jcm6020016.
8. Neunert CE. Current management of immune thrombocytopenia. American Society of Hematology. 2013;2013:276-82.
9. Stasi R. How to approach thrombocytopenia. Am Soc of Hematol. 2012;2012(1): 191-7
10. Wei Y, Ji XB, Wang YW, Wang Jx, Yang EQ, Wang ZC, et al. High-dose dexamethasone vs prednisone for treatment of adult immune thrombocytopenia: A prospective
multicenter randomized trial. Blood. 2016; 127(3):296-302; quiz 370.
11. Bohn JP, Steurer M. Current and evolving treatment strategies in adult immune thrombocytopenia. memo. 2018;11:241-6
12. Roorprai JK, Khamisa K. Is there a role for biweekly romiplostim in the management of chronic immune thrombocytopenia (ITP)? A report of three cases. Case Rep
Hematol. 2018;2018:6037494.
13. George JN. Sequence of treatments for adults with primary immune thrombocytopenia. Am J Hematol. 2012;20(87):12-15
14. Eghbali A, Azadmanesh P, Bagheri B, Taherahmadi H, Sadeghi Sedeh B. Comparison between IV immune globulin (IVIG) and anti-D globulin for treatment of
immune thrombocytopenia: A randomized open-label study. Fundamental Clin Pharmacol. 2016;30(4):385-9.
CDK-280/ vol. 46 no. 11 th. 2019 661
Figure 1: Second-Line Therapies for Adults
Adult with ITP > 3 months
Dependent on or unresponsive
to corticosteroids
3-12 months Assess duration of ITP >12 months
Primary treatment options: Primary treatment options:
Rituximab, TPO-RA Rituximab, Splenectomy,
TPO-RA
Assess patient values Assess patient values
and preferences
Patient places a high Patient places a high Patient places a high Patient places a high Patient places
value on achieving value on avoiding value on achieving value on avoiding a high value on
durable response long-term medication durable response long-term medication avoiding surgery
Treatment options: Treatment options:
TPO-RA Rituximab Treatment options:
Splenectomy, Rituximab,
Rituximab, TPO-RA
TPO-RA Splenectomy
Figure 1. Selection of second-line therapy in adults with Patient Patient Patient Patient Patient Patient
ITP should be individualized based on duration of disease places a places a places a places a places a places a
and patient values and preferences. Other factors that may high high high high high high
value on value on value on value on value on value on
influence treatment decisions include frequency of bleeding
avoiding avoiding avoiding durable achiving avoiding
sufficient to require hospitalization or rescue medication,
surgery long-term surgery response durable long-term
comorbidities, compliance, medical and social support
medication response medication
networks, cost, and availability of treatments. Patient
education and shared decision-making is encouraged.
Patient characteristics
TPO-RA TPO-RA
Splenectomy Splenectomy
Rituximab Rituximab
Actions
Treatment options
TPO-RA – thrombopoietin receptor agonist
All recommendations in Figure 1 are conditional recommendations
Pediatric Second-Line Therapies for Children
In children with ITP lasting ≥3 months who have non-life-threatening
INPATIENT VS. OUTPATIENT MANAGEMENT mucosal bleeding and/or diminished health-related quality of life
Table 3 – Management of Newly Diagnosed ITP and do not respond to first-line treatment, the ASH guideline panel
suggests the following options for second-line therapies presented
Platelet Count Management in the order they should be pursued :
Platelet count of <20 x109/l and no or mild 1. Thrombopoietin receptor agonist (eltrombopag or romiplostim)1
Outpatient1
bleeding (skin manifestations) only 2. Rituximab
Platelet count of ≥20 x109/l and no or mild 3. Splenectomy2
Outpatient1
bleeding (skin manifestations) only 1
Individual patient preference may place a higher value on the use of a daily oral medication (eltrombopag)
or one that requires weekly subcutaneous injections (romiplostim). For pediatric patients, eltrombopag
1
For patients with uncertainty about the diagnosis, those with social concerns, those who live far from the dosing should avoid consumption of calcium containing foods such as dairy products by four hours. This
hospital, or those for whom follow-up cannot be guaranteed, admission to the hospital may be preferable. may limit the ability of some children to take this medication.
2
If possible, splenectomy should be delayed as long as possible after diagnosis because of the potential for
spontaneous remission in the first year.
Good Practice Statement
Patients not admitted to the hospital should receive education and Good Practice Statement
expedited follow-up with a hematologist within 24-72 hours.
The treating physician should ensure that patients have appropriate
immunizations prior to splenectomy and that they receive counseling
regarding antibiotic prophylaxis following splenectomy. The treating
OBSERVATION VS. TREATMENT physician should also educate the patient on prompt recognition and
In children with newly diagnosed ITP who have no or minor bleeding, management of fever and refer to current recommendations on pre- and
the ASH guideline panel recommends observation over both post-splenectomy care.
intravenous immunoglobulin and anti-D immunoglobulin , and
suggests observation over corticosteroids .
Each of the these second-line treatments may be effective therapy
TREATMENT and therefore the choice of treatment should be individualized based
First-Line Therapies for Children on duration of ITP, frequency of bleeding episodes requiring hospi-
talization or rescue medication, comorbidities, adherence, medical
In children with newly diagnosed ITP who have non-life-threatening
and social support networks, patient values and preferences, cost,
mucosal bleeding and/or diminished health-related quality of life, the
and availability. Patient education and shared decision-making are
ASH guideline panel suggests corticosteroids rather than intrave-
encouraged.
nous immunoglobulin or anti-D immunoglobulin1 . For patients where
corticosteroids are contra-indicated or otherwise not preferred, the
ASH guideline panel suggests either intravenous immunoglobulin or
anti-D immunoglobulin2 .
In children with newly diagnosed ITP who have non-life-threatening
mucosal bleeding and/or diminished health related quality of life,
the ASH guideline panel recommends against courses of
corticosteroids longer than 7 days in favor of courses 7 days or
shorter , and suggests prednisone (2 - 4 mg/kg/day; maximum, 120
mg daily, for 5-7 days) rather than dexamethasone (0.6 mg/kg/day;
maximum, 40 mg/kg/day, for 4 days) .
1
This recommendation assumes corticosteroid dosing as outlined in the following paragraph. This recom-
mendation is reserved only for children with non-major mucosal bleeding.
2
This recommendation is reserved only for children with non-major mucosal bleeding
Good Practice Statement
For patients receiving corticosteroids, the treating physician should ensure
the patient is adequately monitored for potential side effects regardless
of the duration or type of corticosteroid selected. This includes close
monitoring for hypertension, hyperglycemia, sleep and mood disturbances,
gastric irritation or ulcer formation, glaucoma, myopathy and osteoporosis.
Given the potential impact of corticosteroids on mental health, the treating
physician should conduct an assessment of health-related quality of life
(HRQoL) (depression, fatigue, mental status etc.) while patients are
receiving corticosteroids.
Strength of Recommendations and Quality of Evidence
The methodology for determining the strength of each recommendation and the quality of the
evidence supporting the recommendations was adapted from GRADE: an emerging consen-
sus on rating quality of evidence and strength of recommendations. Guyatt GH, et al; GRADE
Working Group. 2008;336(7650):924–926. More details on this specific adaptation of the
GRADE process can be found in American Society of Hematology 2019 Guideline for Immune
Thrombocytopenia.1
Strength of Recommendation
Strong recommendations - Most individuals should follow the recommended course of ac-
tion. Formal decision aids are not likely to be needed to help individual patients make decisions
consistent with their values and preferences.
Conditional recommendations - Recognize that different choices will be appropriate for indi-
vidual patients and that you must help each patient arrive at a management decision consistent
with his or her values and preferences. Decision aids may be useful in helping individuals to
make decisions consistent with their individual risks, values and preferences.
How to Use This Pocket Guide
ASH pocket guides are primarily intended to help clinicians make decisions about diagnostic
and treatment alternatives. The information included in this guide is not intended to serve or
be construed as a standard of care. Clinicians must make decisions on the basis of the unique
clinical presentation of an individual patient, ideally though a shared process that considers
the patient’s values and preferences with respect to all options and their possible outcomes.
Decisions may be constrained by realities of a specific clinical setting, including but not limited
to institutional policies, time limitations, or unavailability of treatments. ASH pocket guides may
not include all appropriate methods of care for the clinical scenarios described. As science
advances and new evidence becomes available, these pocket guides may become obsolete.
Following these guidelines cannot guarantee successful outcomes ASH does not warrant or
guarantee any products described in these guidelines.
The complete 2019 ASH Clinical Practice Guideline for Immune Thrombocytopenia1 include
additional remarks and contextual information that may affect clinical decisionmaking. To learn
more about these guidelines, visit hematology.org/ITPguidelines.
Conflict of interest information for Drs. Neunert, Vesely, Mithoowani, and Kim may be found at
hematology.org/pocketguidesCOI.
1
Neunert C, Terrell DR, Arnold DM, et al. American Society of Hematology 2019 guideline for immune
thrombocytopenia. Blood Adv. 2019. In press.
This and other ASH pocket guides are also available in the ASH Pocket
Guides App, available for Android and iOS devices. More information
about this and other ASH pocket guides may be found
at hematology.org/pocketguides.
© 2019 American Society of Hematology
All rights reserved. No part of this publication may be reproduced, stored in a retrieval
system, or transmitted in any form or by any means, electronic or mechanical, including
photocopy, without prior written consent of the American Society of Hematology.
American Society of Hematology
2021 L Street NW, Suite 900
Washington, DC 20036
www.hematology.org
For expert consultation on immune thrombocytopenia and other hematologic questions,
submit a request to the ASH Consult a Colleague program at
www.hematology.org/consult (ASH members only).
Anda mungkin juga menyukai
- Kapita Selekta Kedokteran Edisi IV Jilid 1Dokumen2 halamanKapita Selekta Kedokteran Edisi IV Jilid 1فرجني موغBelum ada peringkat
- Laporan Pendahuluan ItpDokumen8 halamanLaporan Pendahuluan ItpHanda Tri NurcahyoBelum ada peringkat
- Immune ThrombocytopeniaDokumen4 halamanImmune ThrombocytopeniamelchiadiBelum ada peringkat
- Translated Copy of CCD-5-410Dokumen6 halamanTranslated Copy of CCD-5-410syaifulBelum ada peringkat
- Makalah, Translate, - CoverDokumen14 halamanMakalah, Translate, - CoverArdian Zaka RABelum ada peringkat
- Igd Itp WordDokumen5 halamanIgd Itp WordppdsmikroundipBelum ada peringkat
- Dokumen - Tips Idiopathic Trombositopenia Purpura WordDokumen9 halamanDokumen - Tips Idiopathic Trombositopenia Purpura WordMuhammad FahrisBelum ada peringkat
- TROMBOSITOPENIADokumen9 halamanTROMBOSITOPENIAagustinadewiBelum ada peringkat
- ItpDokumen8 halamanItpKhoirul FifahBelum ada peringkat
- ItpDokumen18 halamanItpEurasia BlossomBelum ada peringkat
- Referat ItpDokumen16 halamanReferat ItpNandika Nurfitria100% (1)
- No 6 UfarahDokumen8 halamanNo 6 UfarahUfarah Indah SariBelum ada peringkat
- Drug Induced TrombositopeniaDokumen4 halamanDrug Induced TrombositopeniaRiyan SopiyanBelum ada peringkat
- Idiopatik Trombositopenia PurpuraDokumen6 halamanIdiopatik Trombositopenia PurpuraFarah Basotjatjo KaharBelum ada peringkat
- LP ItpDokumen9 halamanLP ItpZaqiyah ZaqiyahBelum ada peringkat
- Jurnal Kesehatan Mengenai ItpDokumen3 halamanJurnal Kesehatan Mengenai ItpiwanBelum ada peringkat
- Hepatitis C Mempengaruhi Trombosit 2Dokumen7 halamanHepatitis C Mempengaruhi Trombosit 2Gita ParadiseBelum ada peringkat
- Immune Thrombocytopenic Purpura: Oleh DRDokumen39 halamanImmune Thrombocytopenic Purpura: Oleh DRtaufik.abdiBelum ada peringkat
- Asuhan ItpDokumen13 halamanAsuhan ItpDIO ALMASBelum ada peringkat
- Patofisiologi ITPDokumen33 halamanPatofisiologi ITPMichelle Hutahuruk100% (4)
- Asuhan Keperawatan ITPDokumen14 halamanAsuhan Keperawatan ITPNello IndigoBelum ada peringkat
- ItpDokumen19 halamanItpZifa ArdilafBelum ada peringkat
- Referat ITP FixDokumen14 halamanReferat ITP FixarnisaskyaBelum ada peringkat
- Tinjauan Pustaka - ITPDokumen11 halamanTinjauan Pustaka - ITPYolandaBelum ada peringkat
- Idiopathic Thrombocytopenic Purpura Dalam KehamilanDokumen7 halamanIdiopathic Thrombocytopenic Purpura Dalam KehamilanPratita Jati PermatasariBelum ada peringkat
- Itp Bab 2 Konsep DasarDokumen7 halamanItp Bab 2 Konsep DasarRiskiDafiantoBelum ada peringkat
- Referat ITPDokumen20 halamanReferat ITPWindy50% (2)
- ITP Pada AnakDokumen7 halamanITP Pada AnakAlief Abni BernindraBelum ada peringkat
- LP ITP SudiDokumen17 halamanLP ITP SudiLuh SudhiBelum ada peringkat
- Laporan Pendahuluan Itp FixDokumen10 halamanLaporan Pendahuluan Itp FixRizki Faridatul HakikiBelum ada peringkat
- Itp SefiaDokumen4 halamanItp SefiaSeffia RiandiniBelum ada peringkat
- LP ItpDokumen18 halamanLP ItpChibee Siie Saraph Part IIBelum ada peringkat
- Idiopatik Trombositopenia PurpuraDokumen24 halamanIdiopatik Trombositopenia PurpuraMuhamad SyaifulBelum ada peringkat
- Purpura Trombositopenia IdiopatikDokumen5 halamanPurpura Trombositopenia IdiopatikRani MuliaBelum ada peringkat
- Trombositopenia Purpura IdiopatikDokumen6 halamanTrombositopenia Purpura Idiopatikkmardhiyah100% (1)
- Ideopatik Trombositopenia PurpuraDokumen10 halamanIdeopatik Trombositopenia Purpurarian0877Belum ada peringkat
- Review Tugas Buk EfridaDokumen12 halamanReview Tugas Buk EfridaAnonymous lVfqKMlyXBelum ada peringkat
- CRS ItpDokumen24 halamanCRS ItpHafizhDzaki24 ChannelBelum ada peringkat
- TROMBOSITOPENIADokumen7 halamanTROMBOSITOPENIAJonas SihombingBelum ada peringkat
- Immune Thrombocytopenic PurpuraDokumen4 halamanImmune Thrombocytopenic PurpuraemmyBelum ada peringkat
- LP ItpDokumen13 halamanLP ItpJimi FaqihBelum ada peringkat
- Referat ItpDokumen23 halamanReferat ItpAnggie Nisa Nur'aeni100% (1)
- ITPDokumen11 halamanITPLili PutriBelum ada peringkat
- Referat TrombositopeniaDokumen11 halamanReferat TrombositopeniaMellyBelum ada peringkat
- Summary IPDDokumen34 halamanSummary IPDVaza NadiaBelum ada peringkat
- Idiopathic TPDokumen10 halamanIdiopathic TPEviner AsengBelum ada peringkat
- Itp Pada Anak (KLMPK 3)Dokumen13 halamanItp Pada Anak (KLMPK 3)Lyra Make UpBelum ada peringkat
- Itp Pada Anak (KLMPK 3)Dokumen13 halamanItp Pada Anak (KLMPK 3)Lyra Make UpBelum ada peringkat
- Adoc - Pub Bab I Pendahuluan Bab II 1Dokumen21 halamanAdoc - Pub Bab I Pendahuluan Bab II 1Nadya Indah SariBelum ada peringkat
- UntitledDokumen33 halamanUntitledFrans SiraitBelum ada peringkat
- Laporan Pendahuluan ItpDokumen3 halamanLaporan Pendahuluan ItpVinista R. KiranaBelum ada peringkat
- Disseminated Intravascular CoagulationDokumen21 halamanDisseminated Intravascular CoagulationTomyBelum ada peringkat
- Penanganan Terkini Idiopatik Trombositopenia PurpuraDokumen12 halamanPenanganan Terkini Idiopatik Trombositopenia PurpuraKhristina 'dama-damay'Belum ada peringkat
- Idiopathic Trombositopenia Purpura WordDokumen9 halamanIdiopathic Trombositopenia Purpura WordNerhis Sydney WisakaBelum ada peringkat
- Mikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaDari EverandMikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaPenilaian: 2.5 dari 5 bintang2.5/5 (2)
- Mikrobiologi Medis I: Patogen dan Mikrobioma ManusiaDari EverandMikrobiologi Medis I: Patogen dan Mikrobioma ManusiaPenilaian: 4 dari 5 bintang4/5 (11)