Anda mungkin juga menyukai
- Elektro Fisika Dan Sumber Fisis 2 Pertemuan 1aDokumen37 halamanElektro Fisika Dan Sumber Fisis 2 Pertemuan 1aRachmat BayuBelum ada peringkat
- THERMOTHERAPY AND CRYOTHERAPY (Terapi Panas Dan TerapiDokumen28 halamanTHERMOTHERAPY AND CRYOTHERAPY (Terapi Panas Dan TerapiFajar AhsanBelum ada peringkat
- Cryotherapy Dan HydrotherapyDokumen20 halamanCryotherapy Dan Hydrotherapy23.NiLuhPutu Dona MahaYantiBelum ada peringkat
- Modalitas ElektroterapiDokumen63 halamanModalitas ElektroterapiNurfatri Ramadani50% (2)
- PK Bu VennyDokumen4 halamanPK Bu VennydiantriramadhaniBelum ada peringkat
- Cryotherapy DLM FTDokumen24 halamanCryotherapy DLM FTGaluh Dwinanda IIBelum ada peringkat
- Thermo TherapyDokumen4 halamanThermo TherapyrikamaulidaBelum ada peringkat
- Terapi Panas DinginDokumen9 halamanTerapi Panas DinginprasetyaningsihBelum ada peringkat
- Materi HydrotherapyDokumen11 halamanMateri HydrotherapyFaisal RuhiatnaBelum ada peringkat
- Tugas FT or Paper DimasHDokumen5 halamanTugas FT or Paper DimasHDimas HikamBelum ada peringkat
- Suhu TubuhDokumen40 halamanSuhu TubuhAhmad FauzinorBelum ada peringkat
- Terapi Dingin (Cold Therapy) Dalam Penanganan Cedera OlahragaDokumen11 halamanTerapi Dingin (Cold Therapy) Dalam Penanganan Cedera OlahragaSyamsofian SyamsuddinBelum ada peringkat
- Kuliah MODALITASDokumen70 halamanKuliah MODALITASDitha OsokBelum ada peringkat
- Kuliah MODALITASDokumen58 halamanKuliah MODALITASAgusBelum ada peringkat
- Kompres Panas DinginDokumen18 halamanKompres Panas Dinginberthy koupunBelum ada peringkat
- Cold TherapyDokumen31 halamanCold TherapyomboBelum ada peringkat
- Cold BathDokumen26 halamanCold BathRahmadanii RahmadaniiBelum ada peringkat
- Kompres Panas DinginDokumen21 halamanKompres Panas DinginedvistaBelum ada peringkat
- Kompres Air Hangat Dan DinginDokumen26 halamanKompres Air Hangat Dan DinginfikaBelum ada peringkat
- Rangkuman Bab 4 Thermotheraphy Restu Rifaldi-P22030119042Dokumen9 halamanRangkuman Bab 4 Thermotheraphy Restu Rifaldi-P22030119042RESTU RIFALDI mhsD4TEM2019BBelum ada peringkat
- Shivering Post OpDokumen12 halamanShivering Post Opsupit10% (1)
- Terapi DinginDokumen21 halamanTerapi DinginImhaBelum ada peringkat
- Terapi DinginDokumen21 halamanTerapi DinginInggriht Senny BondangBelum ada peringkat
- Kompres Panas DinginDokumen49 halamanKompres Panas DinginEndang rahayuBelum ada peringkat
- Translate KLP 11 HydroDokumen69 halamanTranslate KLP 11 HydrosuciBelum ada peringkat
- Sistem Termoregulasi: Interthreshold Range Merupakan Skala Respon Termoregulator Terhadap Dingin Atau Panas. JikaDokumen10 halamanSistem Termoregulasi: Interthreshold Range Merupakan Skala Respon Termoregulator Terhadap Dingin Atau Panas. JikaTia ListyanaBelum ada peringkat
- Efek Fisiologis Dan Terapeutik Sinar Infra MerahDokumen6 halamanEfek Fisiologis Dan Terapeutik Sinar Infra MerahFadil RamadhanBelum ada peringkat
- Heating External-1Dokumen18 halamanHeating External-1NI KETUT NOVIANI SUWANTIBelum ada peringkat
- Modalitas Therapy OrthopedicDokumen31 halamanModalitas Therapy Orthopedicihwan Ukhrawi AlyBelum ada peringkat
- Cold Heat TherapyDokumen16 halamanCold Heat TherapyAvira Berlianna SalsaBelum ada peringkat
- Cold and Heat TherapyDokumen17 halamanCold and Heat Therapylove tripBelum ada peringkat
- Protap Sumber FisisDokumen10 halamanProtap Sumber FisisRezki Ayu ParadillahBelum ada peringkat
- Bahan ShiveringDokumen4 halamanBahan ShiveringYusa Has JulianaBelum ada peringkat
- Kompres Panas DinginDokumen23 halamanKompres Panas DinginFeno Suci WulandariBelum ada peringkat
- Tugas Fisika Fisioterapi - Yudith Leo Bantara - J120210198 - C-DikonversiDokumen2 halamanTugas Fisika Fisioterapi - Yudith Leo Bantara - J120210198 - C-DikonversiCarl JohnsonBelum ada peringkat
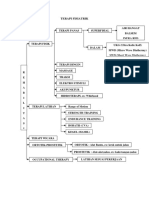
- Terapi FisiatrikDokumen25 halamanTerapi FisiatrikAstie NomleniBelum ada peringkat
- MAKALAH Terapi Dingin (Cold Therapy)Dokumen15 halamanMAKALAH Terapi Dingin (Cold Therapy)Hardianti Putri DianBelum ada peringkat
- Literature Kompres 2Dokumen7 halamanLiterature Kompres 2echaBelum ada peringkat
- LongneckerDokumen2 halamanLongneckerTia ListyanaBelum ada peringkat
- Laporan Praktikum MWDDokumen7 halamanLaporan Praktikum MWDIsyaturradiahBelum ada peringkat
- Panas (Fisika Kesehatan) JuliDokumen35 halamanPanas (Fisika Kesehatan) JuliYulian LoupattyBelum ada peringkat
- TERAPI FISIATRIK, Dari Slide 1-16, DinginDokumen34 halamanTERAPI FISIATRIK, Dari Slide 1-16, DinginAchmad Nur AffendickBelum ada peringkat
- Resume Kompres InayahDokumen17 halamanResume Kompres InayahInayah RahmaBelum ada peringkat
- Hidro Terapi-1Dokumen6 halamanHidro Terapi-1irdaBelum ada peringkat
- TERMODINAMIKA2Dokumen49 halamanTERMODINAMIKA2Primadanie Rengganis MdfBelum ada peringkat
- Laporan ReadingDokumen56 halamanLaporan ReadingTania ARBelum ada peringkat
- Mekanisme ShiveringDokumen25 halamanMekanisme ShiveringAnonymous 46SyYMQkBelum ada peringkat
- Tugas Individu Kepdas Ghia Septya Hardi 25bDokumen7 halamanTugas Individu Kepdas Ghia Septya Hardi 25bGhia 69Belum ada peringkat
- Kuliah Termoregulasi-D3 KebidananDokumen35 halamanKuliah Termoregulasi-D3 KebidanantrisiaBelum ada peringkat
- Aplikasi Ft. Modalitas Air Dan GasDokumen12 halamanAplikasi Ft. Modalitas Air Dan GasDinda Ayu Putri DevaniBelum ada peringkat
- Hipotermia Dan AnestesiDokumen11 halamanHipotermia Dan AnestesiazisfitriBelum ada peringkat
- MENGGIGILDokumen9 halamanMENGGIGILhari sBelum ada peringkat
- KLP 5 Heat CrampsDokumen9 halamanKLP 5 Heat CrampsAyu AristiaBelum ada peringkat
- Pengaturan SuhuDokumen46 halamanPengaturan SuhuAnisya Ulfah HanumBelum ada peringkat
- Bab 52-MorganDokumen15 halamanBab 52-MorganJurnal inBelum ada peringkat
- Pertemuan 2 - TermofisikaDokumen21 halamanPertemuan 2 - Termofisikabela novitaBelum ada peringkat
- Laporan Biofisik Panas, Dingin Dan HidrotherapiDokumen13 halamanLaporan Biofisik Panas, Dingin Dan HidrotherapiAndi Nurung TulnisaBelum ada peringkat
- Calcaneus Spur FixxDokumen31 halamanCalcaneus Spur FixxAmethysa DiaryBelum ada peringkat
- Group Group Group: Nomer Meja 3 Nomer Meja 01Dokumen2 halamanGroup Group Group: Nomer Meja 3 Nomer Meja 01Amethysa Diary100% (1)
- 4644 1. Manajemen FT Pada Fracture CervicalisDokumen93 halaman4644 1. Manajemen FT Pada Fracture CervicalisAmethysa DiaryBelum ada peringkat
- Fraktur Colles Dan Supracondylar HumerusDokumen50 halamanFraktur Colles Dan Supracondylar HumerusAmethysa DiaryBelum ada peringkat
- NumberDokumen20 halamanNumberMuhimmatul Khoiroh100% (1)
- Matching WorksheetDokumen46 halamanMatching WorksheetMuhimmatul KhoirohBelum ada peringkat
- Skkni 2018-149Dokumen289 halamanSkkni 2018-149bujang angin75% (4)
- Kognitif&Persepsi VisualDokumen37 halamanKognitif&Persepsi VisualAmethysa DiaryBelum ada peringkat
- Perpres 2008 034Dokumen6 halamanPerpres 2008 034Noor SanuriBelum ada peringkat
- Surat Lamaran IrmaDokumen1 halamanSurat Lamaran IrmaAmethysa DiaryBelum ada peringkat
- Surat Lamaran IrmaDokumen1 halamanSurat Lamaran IrmaAmethysa DiaryBelum ada peringkat