Anda mungkin juga menyukai
- Program Pencegahan dan Penyembuhan Skoliosis Untuk AndaDari EverandProgram Pencegahan dan Penyembuhan Skoliosis Untuk AndaPenilaian: 4 dari 5 bintang4/5 (9)
- Jurnal Perawatan Skoliosis Natural Anda: Petunjuk per hari selama 12 minggu untuk tulang belakang yang lebih lurus dan kuat!Dari EverandJurnal Perawatan Skoliosis Natural Anda: Petunjuk per hari selama 12 minggu untuk tulang belakang yang lebih lurus dan kuat!Penilaian: 4.5 dari 5 bintang4.5/5 (7)
- Surat Keterangan Dokter Penyakit Dan Gagal GinjalDokumen5 halamanSurat Keterangan Dokter Penyakit Dan Gagal GinjalIndo JeepBelum ada peringkat
- SURAT KETERANGAN DOKTER HIV KARENA TRANSFUSI DARAH Atau PEKERJAAN FULL BLOWN AIDS HEPATITIS B Atau C KARENA PEKERJAANDokumen6 halamanSURAT KETERANGAN DOKTER HIV KARENA TRANSFUSI DARAH Atau PEKERJAAN FULL BLOWN AIDS HEPATITIS B Atau C KARENA PEKERJAANBandit BanditBelum ada peringkat
- Surat Keterangan Dokter Komplikasi Diabetes Diabetes Melitus Yang Bergantung InsulinDokumen4 halamanSurat Keterangan Dokter Komplikasi Diabetes Diabetes Melitus Yang Bergantung InsulinRISWAN AZHARIBelum ada peringkat
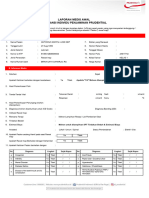
- Laporan Medis Awal Asuransi Individu Penjaminan Prudential: A. Identitas PasienDokumen3 halamanLaporan Medis Awal Asuransi Individu Penjaminan Prudential: A. Identitas PasienfokaliwatesBelum ada peringkat
- Surat Keterangan Dokter Stroke Pembedahan Aneurisma Otak Operasi Otak Hidrosefalus Pemasangan Cerebral ShuntDokumen5 halamanSurat Keterangan Dokter Stroke Pembedahan Aneurisma Otak Operasi Otak Hidrosefalus Pemasangan Cerebral ShuntHerlambang PermadiBelum ada peringkat
- Lma Antonius Manyu, A.md KepDokumen2 halamanLma Antonius Manyu, A.md KepI G. A. Ratna DewiBelum ada peringkat
- CI Surat Keterangan Dokter Untuk Burn Anemia Cancer Medullary CysticDokumen3 halamanCI Surat Keterangan Dokter Untuk Burn Anemia Cancer Medullary CysticDian SyahBelum ada peringkat
- Surat Keterangan Dokter Penyakit JantungDokumen5 halamanSurat Keterangan Dokter Penyakit JantungHary Yudha PrasetiaBelum ada peringkat
- Surat Keterangan Dokter (Major Head Trauma (Stroke)Dokumen6 halamanSurat Keterangan Dokter (Major Head Trauma (Stroke)sisilia sianturiBelum ada peringkat
- Surat Keterangan Dokter Penyakit Kanker Metastasis Otak KDokumen6 halamanSurat Keterangan Dokter Penyakit Kanker Metastasis Otak KSyifa NailaBelum ada peringkat
- 03.cancer 30062015Dokumen4 halaman03.cancer 30062015muhafidBelum ada peringkat
- Surat KonfirmasiDokumen1 halamanSurat Konfirmasiinformasi bundamargoBelum ada peringkat
- Formulir Klaim Penyakit Paru KronisDokumen5 halamanFormulir Klaim Penyakit Paru KronisOrang BaikBelum ada peringkat
- Askep Ibs FixDokumen28 halamanAskep Ibs FixEndrie KhotijahBelum ada peringkat
- Longcase Dan Minicex IcuDokumen25 halamanLongcase Dan Minicex IcuNovita100% (1)
- FWD 230721155540Dokumen9 halamanFWD 230721155540Ilham WahyudiBelum ada peringkat
- Surat Keterangan Dokter Demam RematikDokumen3 halamanSurat Keterangan Dokter Demam RematikCell C35Belum ada peringkat
- B20 Surat GT Kepada GubernurDokumen25 halamanB20 Surat GT Kepada GubernurIchwan Al-KalibataniBelum ada peringkat
- Formulir Klaim DeafnessDokumen4 halamanFormulir Klaim Deafnessplaystation030788Belum ada peringkat
- Nurrohim - 1902080 - Resume 3 - IbsDokumen16 halamanNurrohim - 1902080 - Resume 3 - IbsnurrohimBelum ada peringkat
- Resume HD CKDDokumen12 halamanResume HD CKDredi nakanoBelum ada peringkat
- LmaDokumen1 halamanLmainformasi bundamargoBelum ada peringkat
- Formulir Klaim Dokter Rawat Inap I Rawat Jalan Asuransi KesehatanDokumen3 halamanFormulir Klaim Dokter Rawat Inap I Rawat Jalan Asuransi KesehatanMartunis Alnura AmdKep CHtBelum ada peringkat
- LK KGD Fraktur Rizal-1Dokumen20 halamanLK KGD Fraktur Rizal-1Al OBelum ada peringkat
- RESUM IBS FR MandibulaDokumen22 halamanRESUM IBS FR MandibulaDwi PurwantoBelum ada peringkat
- Asuhan Keperawatan Medikal BedahDokumen18 halamanAsuhan Keperawatan Medikal Bedahseni putri d4 kepBelum ada peringkat
- Handoko - p1337420920077 - Laporan Kasus Minggu IIDokumen20 halamanHandoko - p1337420920077 - Laporan Kasus Minggu IIdexadiazBelum ada peringkat
- Pengkajian Populasi KhususDokumen4 halamanPengkajian Populasi KhususSuci Imbar PratiwiBelum ada peringkat
- Resume HD 2 LutfiDokumen6 halamanResume HD 2 Lutfietam guyonBelum ada peringkat
- Safety CheklistDokumen2 halamanSafety Cheklistdeniro juniorBelum ada peringkat
- LK FamDokumen30 halamanLK FamNeni100% (1)
- ASKEP PERIOPERATIF (SDKI) JesiscaDokumen35 halamanASKEP PERIOPERATIF (SDKI) JesiscaMaria Natalia PongaBelum ada peringkat
- Formulir Identifikasi Kasus Di PuskesmasDokumen3 halamanFormulir Identifikasi Kasus Di PuskesmasIwan RobbyBelum ada peringkat
- Doris Natalia 100822 RSDCDokumen9 halamanDoris Natalia 100822 RSDCmadityas_777Belum ada peringkat
- Avrist-Formulir Keterangan Medis Cacat Total Dan TetapDokumen3 halamanAvrist-Formulir Keterangan Medis Cacat Total Dan TetapWindaBelum ada peringkat
- 3B - 073 - Meiliani Uswatun KH - Tugas Kep PaliatifDokumen11 halaman3B - 073 - Meiliani Uswatun KH - Tugas Kep PaliatifMeiliani Uswatun KhasanahBelum ada peringkat
- Askep RSK AsokaDokumen40 halamanAskep RSK AsokaMina watiBelum ada peringkat
- 1 Askep CvaDokumen21 halaman1 Askep Cvavivi alvionitaBelum ada peringkat
- Askep Devita NazwaDokumen11 halamanAskep Devita NazwaMoch AnggaraBelum ada peringkat
- Laporan Resume 2 IKODokumen41 halamanLaporan Resume 2 IKODwi PurwantoBelum ada peringkat
- Formulir Allianz Penyakit Kritis SLEDokumen5 halamanFormulir Allianz Penyakit Kritis SLEAquilando David Mario SimatupangBelum ada peringkat
- 1 Master FormDokumen2 halaman1 Master FormRina TeweBelum ada peringkat
- Soap Reproduksi Nu NeliDokumen9 halamanSoap Reproduksi Nu NeliRoslin SitorusBelum ada peringkat
- Askep DMDokumen14 halamanAskep DMdiana syafaBelum ada peringkat
- KUESIONER KEHAMILAN (A4) 2 Lembar SQS (Baru) PDFDokumen2 halamanKUESIONER KEHAMILAN (A4) 2 Lembar SQS (Baru) PDFKhoirul AlhakimBelum ada peringkat
- Form PeDokumen2 halamanForm PeIRWAN FARIDBelum ada peringkat
- Formulir Klain Rawat InapDokumen3 halamanFormulir Klain Rawat Inaphanung.wicaksonoBelum ada peringkat
- TPD Confidential Medical Certificate - 201910 - FinalDokumen7 halamanTPD Confidential Medical Certificate - 201910 - FinalnavinBelum ada peringkat
- LK Irna1 B TN.SDokumen28 halamanLK Irna1 B TN.SIntan SafirahBelum ada peringkat
- LK LaparatomiDokumen13 halamanLK Laparatomiazza koharBelum ada peringkat
- Askep BPHDokumen16 halamanAskep BPHMirzon AltafBelum ada peringkat
- Askep Gadar Elisa Ana SafitriDokumen20 halamanAskep Gadar Elisa Ana SafitriMemelBelum ada peringkat
- Askep Stroke HemoragikDokumen5 halamanAskep Stroke HemoragikZeasly Tiofenly NeolakaBelum ada peringkat
- Askep Devita NazwaDokumen11 halamanAskep Devita NazwaMoch AnggaraBelum ada peringkat
- Resume Ok NurhaniDokumen12 halamanResume Ok NurhaniNurllia SalamaBelum ada peringkat
- Tumor MamaDokumen6 halamanTumor MamaEtho SoiBelum ada peringkat
- ASKEPDokumen16 halamanASKEPviolitakpBelum ada peringkat
- Askep Ujian Kista Ovarium-Itsnaini Wahyu-P137420921134Dokumen14 halamanAskep Ujian Kista Ovarium-Itsnaini Wahyu-P137420921134Khadirotunumrifauzi UmriafBelum ada peringkat