Anda mungkin juga menyukai
- Desain Inovatif Bu IsriDokumen20 halamanDesain Inovatif Bu Isrikomite keperawatanBelum ada peringkat
- DRK Keperawatan KritisDokumen48 halamanDRK Keperawatan KritisDesy Simarmata100% (1)
- Logbook PK Gadar & Kritis Ners FixDokumen49 halamanLogbook PK Gadar & Kritis Ners FixDwiputri YuliantiBelum ada peringkat
- Keripik TalesDokumen20 halamanKeripik TalesKukuh BakatBelum ada peringkat
- Kebijakan KTD SentinelDokumen4 halamanKebijakan KTD SentinelimmawatiBelum ada peringkat
- Tool UkomDokumen2 halamanTool UkomBudi SasmitaBelum ada peringkat
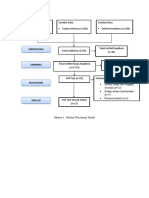
- Skema Pencarian JurnalDokumen1 halamanSkema Pencarian JurnalIhsan EooiBelum ada peringkat
- K3 SehatDokumen202 halamanK3 SehatfarizBelum ada peringkat
- Tugas Analisa Jurnal Dengan PICODokumen8 halamanTugas Analisa Jurnal Dengan PICORina InaBelum ada peringkat
- Mankep Hitung KetenagaanDokumen81 halamanMankep Hitung KetenagaanGina CarolineBelum ada peringkat
- Makalah Keperawatan JiwaDokumen24 halamanMakalah Keperawatan JiwaNisa ArianaBelum ada peringkat
- SkripsiDokumen100 halamanSkripsisepriBelum ada peringkat
- Struktur Data Dan Algoritma PDF FreeDokumen119 halamanStruktur Data Dan Algoritma PDF FreeKhanif FaoziBelum ada peringkat
- Formulir Risk Register 2018Dokumen20 halamanFormulir Risk Register 2018Ayu KarinaBelum ada peringkat
- Pra Ukom PerawatDokumen32 halamanPra Ukom PerawatBudi HartonoBelum ada peringkat
- Laporan MOD 5Dokumen102 halamanLaporan MOD 5Rizky Nur UtomoBelum ada peringkat
- Proposal Elin Bab 1-4 PDFDokumen65 halamanProposal Elin Bab 1-4 PDFElin NurannisaBelum ada peringkat
- Pak Spondilitis TBDokumen2 halamanPak Spondilitis TByenni elfiraBelum ada peringkat
- Konsep Keperawatan Gawat DaruratDokumen25 halamanKonsep Keperawatan Gawat DaruratAzalikaIrsantiPutri100% (1)
- Model Kualiatas UdaraDokumen41 halamanModel Kualiatas UdaraFaizBelum ada peringkat
- Manajemen Stategik Dalam TindakanDokumen38 halamanManajemen Stategik Dalam TindakanNorlinBelum ada peringkat
- Blue PrintDokumen16 halamanBlue Printpurnawan0% (1)
- Pengaruh Budaya Organisasi Terhadap Kinerja Tim Dalam Penerapan Patient Safety Di RS Ibnu Sina Makassar PDFDokumen240 halamanPengaruh Budaya Organisasi Terhadap Kinerja Tim Dalam Penerapan Patient Safety Di RS Ibnu Sina Makassar PDFAgus TaufiqBelum ada peringkat
- Xxari Wijaya-162310101276Dokumen96 halamanXxari Wijaya-162310101276Tinna Puspita Marita SariBelum ada peringkat
- Analisi Kasus Kel. JDokumen20 halamanAnalisi Kasus Kel. JWidya AnggraeniBelum ada peringkat
- Indikator Mutu Mcu 2022 FixDokumen3 halamanIndikator Mutu Mcu 2022 FixMeizar TriwardhaniBelum ada peringkat
- Form Pengkajian IGDDokumen7 halamanForm Pengkajian IGDEL Maria UlfaBelum ada peringkat
- 2.2 Proker - Keamanan - 2022Dokumen10 halaman2.2 Proker - Keamanan - 2022Anastasia NimasBelum ada peringkat
- Analisa Risiko Secara Proaktif (FMEA)Dokumen45 halamanAnalisa Risiko Secara Proaktif (FMEA)Mutia FafaBelum ada peringkat
- LK Lengkap FrakturDokumen26 halamanLK Lengkap Frakturyuni ratna12s100% (1)
- Inovasi FixDokumen17 halamanInovasi FixseppurnamaBelum ada peringkat
- Penetapan Indikator Mutu Pelayanan RSB AsihDokumen22 halamanPenetapan Indikator Mutu Pelayanan RSB AsihEka SetiyantoBelum ada peringkat
- Sop Drum BuisDokumen2 halamanSop Drum BuismubramBelum ada peringkat
- Laporan KFA TramadolDokumen10 halamanLaporan KFA Tramadolkiki hardiantiBelum ada peringkat
- Proker 2023 Ruang Rawat InapDokumen71 halamanProker 2023 Ruang Rawat InapyoezufBelum ada peringkat
- Formulir Kredensialing BPJS PDFDokumen45 halamanFormulir Kredensialing BPJS PDFcitra husadaBelum ada peringkat
- ID Analisis Beban Kerja Tenaga Perawat Di IDokumen11 halamanID Analisis Beban Kerja Tenaga Perawat Di IveronicaBelum ada peringkat
- Analisis Kinerja Perawat - Jurnal PDFDokumen21 halamanAnalisis Kinerja Perawat - Jurnal PDFPenarikaBelum ada peringkat
- Bahan Ajar Konstruksi GeometrisDokumen10 halamanBahan Ajar Konstruksi GeometrisnakbiakBelum ada peringkat
- Form Laporan Lab Staf TerpaparDokumen1 halamanForm Laporan Lab Staf Terpaparsri wahyuniBelum ada peringkat
- 2 Pedoman Pelayanan Irna Publik - Final Fix 2022 - 0Dokumen46 halaman2 Pedoman Pelayanan Irna Publik - Final Fix 2022 - 0Talenta BaregaBelum ada peringkat
- Kata Pengantar Daftar IsiDokumen2 halamanKata Pengantar Daftar IsiTien VanenssiaBelum ada peringkat
- Penkes Pemberian ImunisasiDokumen9 halamanPenkes Pemberian Imunisasieko jaeniBelum ada peringkat
- Laporan Root Cause AnalysisDokumen23 halamanLaporan Root Cause AnalysisArtana Sayoga100% (1)
- EKG (Elektrokardiogram)Dokumen27 halamanEKG (Elektrokardiogram)vira100% (1)
- Kontingensi Plan Arus Pasien Terhambat Yang Dari IGDDokumen4 halamanKontingensi Plan Arus Pasien Terhambat Yang Dari IGDWina MarlinBelum ada peringkat
- Kuisioner Kepuasan PelangganDokumen3 halamanKuisioner Kepuasan PelangganDyna KusumaningrumBelum ada peringkat
- Bab 1-4 Mini Riset Rsud NWDokumen59 halamanBab 1-4 Mini Riset Rsud NWUnah NanaBelum ada peringkat
- JCI Survey Process Guide 6th Edition - IND PDFDokumen193 halamanJCI Survey Process Guide 6th Edition - IND PDFRDII YANMEDRSDS100% (2)
- CR Internal Audit Bab 6Dokumen12 halamanCR Internal Audit Bab 6Amelia Salsabila EkasariBelum ada peringkat
- 20 Pengoperasian Dan Pemeliharaan Central MonitorDokumen2 halaman20 Pengoperasian Dan Pemeliharaan Central MonitorzekyBelum ada peringkat
- Monitoring Pasien HemodialisaDokumen2 halamanMonitoring Pasien HemodialisaLannosiibocahpeskins DorksZilla100% (1)
- Proker Lab 2018 (Word)Dokumen21 halamanProker Lab 2018 (Word)mamahosieleBelum ada peringkat
- Tugas Makp Rs Paru PamekasanDokumen83 halamanTugas Makp Rs Paru PamekasanandyekabachtiarBelum ada peringkat
- Profile Imut PERINADokumen15 halamanProfile Imut PERINALogistik Bekasi TimurBelum ada peringkat
- ROOT CAUSE ANALYSIS (RCA) Contoh KasusDokumen12 halamanROOT CAUSE ANALYSIS (RCA) Contoh KasusentangBelum ada peringkat
- Lina Solihan (Gangguan Rasa Nyaman Nyeri)Dokumen36 halamanLina Solihan (Gangguan Rasa Nyaman Nyeri)lina solihan100% (1)
- Kan SMBL - Transisi 35001ningsih - FinalDokumen38 halamanKan SMBL - Transisi 35001ningsih - Finaliwan prasetyoBelum ada peringkat
- System Penilaian Derajat TraumaDokumen13 halamanSystem Penilaian Derajat Traumanyu2n88100% (3)
- Makalah The New Trauma ScoreDokumen13 halamanMakalah The New Trauma Scorenora yuliani azizahBelum ada peringkat
- SPO Kebutuhan Transportaso PasienDokumen3 halamanSPO Kebutuhan Transportaso PasienRetnoBelum ada peringkat
- Spo Pembersihan AmbulanceDokumen2 halamanSpo Pembersihan AmbulanceRetnoBelum ada peringkat
- SAP Perawatan Luka DMDokumen10 halamanSAP Perawatan Luka DMRetnoBelum ada peringkat
- Ebp Pijat Oksitosin RampuuuuuunggggggggDokumen31 halamanEbp Pijat Oksitosin RampuuuuuunggggggggRetnoBelum ada peringkat
- PROSEDUR KHUSUS Pencabutan KukuDokumen2 halamanPROSEDUR KHUSUS Pencabutan KukuRetnoBelum ada peringkat
- 04 Bab I-V Terapi BermainDokumen23 halaman04 Bab I-V Terapi BermainRetnoBelum ada peringkat
- Prosdur Khusus RJPDokumen4 halamanProsdur Khusus RJPRetnoBelum ada peringkat
- Askep Sehat JiwaDokumen10 halamanAskep Sehat JiwaRetnoBelum ada peringkat
- LP KekDokumen11 halamanLP KekRetnoBelum ada peringkat