Anda mungkin juga menyukai
- Nervus Medianus, Radialis, UlnarisDokumen8 halamanNervus Medianus, Radialis, Ulnarisrizkauliaher100% (2)
- Penatalaksanaan Frozen Shoulder FisioterapiDokumen25 halamanPenatalaksanaan Frozen Shoulder FisioterapiMEDICAL MXBelum ada peringkat
- PEMERIKSAANDokumen3 halamanPEMERIKSAANrosalinaBelum ada peringkat
- HNP 56Dokumen36 halamanHNP 56tari puriBelum ada peringkat
- Pemeriksaan Pada TOS Kelompok 2Dokumen4 halamanPemeriksaan Pada TOS Kelompok 2Setio Dwi AtmojoBelum ada peringkat
- Drop Foot IqbalDokumen31 halamanDrop Foot IqbalDyana Pastria UtamiBelum ada peringkat
- Tendinitis SupraspinatusDokumen19 halamanTendinitis SupraspinatusTheresia Sonya RahardiantyBelum ada peringkat
- 4, Drawer TestDokumen3 halaman4, Drawer TestAnonymous 5vrsB8ITgBelum ada peringkat
- PENATALAKSANAAN Fisioterapi Pada Bells PalsyDokumen31 halamanPENATALAKSANAAN Fisioterapi Pada Bells PalsyFinaNurInsiyah75% (4)
- Laporan Ottawa Rules & Diagnosis, Terapi, Rehab Angkle SprainDokumen7 halamanLaporan Ottawa Rules & Diagnosis, Terapi, Rehab Angkle SprainDhia Adhi PerwirawatiBelum ada peringkat
- Pemeriksaan Spesifik: 1. Yergason's TestDokumen13 halamanPemeriksaan Spesifik: 1. Yergason's TestMhya Karmila OpctBelum ada peringkat
- Ft. Muskuloskeletal Kelompok Fraktur PatellaDokumen13 halamanFt. Muskuloskeletal Kelompok Fraktur Patellarida hayati100% (1)
- Spondylosis LumbalisDokumen14 halamanSpondylosis LumbalisWinda Ari PrehatyaniBelum ada peringkat
- Fisioterapi Pada StrokeDokumen5 halamanFisioterapi Pada Strokeandhikaarie100% (2)
- Cervical Root SyndromeDokumen23 halamanCervical Root SyndromemariniBelum ada peringkat
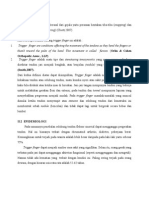
- Trigger FingerDokumen8 halamanTrigger FingerConnyManopeConnyBelum ada peringkat
- Lapsus PLeksus BrachialisDokumen23 halamanLapsus PLeksus BrachialisGibrael JirehBelum ada peringkat
- Lesi N. Tibialis Anterior, Lesi N. Musculocutaneus, Tarsal Tunnel SyndromeDokumen9 halamanLesi N. Tibialis Anterior, Lesi N. Musculocutaneus, Tarsal Tunnel SyndromegravyBelum ada peringkat
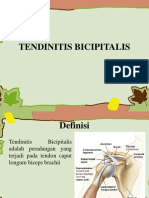
- Tendinitis BicipitalisDokumen71 halamanTendinitis BicipitalisDina Dinda Restiwi100% (1)
- Medial Epicondylitis Test/Golfer Elbow TestDokumen1 halamanMedial Epicondylitis Test/Golfer Elbow TestAditya Josua ElvonBelum ada peringkat
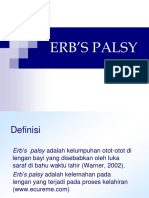
- Erb's PalsyDokumen21 halamanErb's PalsyVthree KyoulBelum ada peringkat
- Makalah IschialgiaDokumen5 halamanMakalah IschialgiaMaria Monica AMS100% (1)
- Dermatom MiotomDokumen29 halamanDermatom MiotomGray Fullbuster100% (3)
- Presus CTS NeuroDokumen22 halamanPresus CTS NeuroDeana MonicaBelum ada peringkat
- Laporan Kasus IDokumen26 halamanLaporan Kasus ISyaema MaulidaBelum ada peringkat
- CL TortikolisDokumen16 halamanCL TortikolisRaihan LuthfiBelum ada peringkat
- No EditDokumen24 halamanNo EditDwita Maya PuspitaBelum ada peringkat
- TentirDokumen9 halamanTentirAde IrmaBelum ada peringkat
- SLAP LesionsDokumen6 halamanSLAP LesionsImron RosadiBelum ada peringkat
- Chedoke MC MasterDokumen18 halamanChedoke MC MasterYeremia YogiBelum ada peringkat
- Myofascial Trigger Point SyndromeDokumen4 halamanMyofascial Trigger Point SyndromeMeis MalirmaseleBelum ada peringkat
- STATUS KASUS Fraktur Colum FemurDokumen14 halamanSTATUS KASUS Fraktur Colum FemuryayaseptianaBelum ada peringkat
- Rheumatoid Arthritis Kelompok 3Dokumen28 halamanRheumatoid Arthritis Kelompok 3Egie ParamarthaBelum ada peringkat
- Piriformis SyndromeDokumen18 halamanPiriformis SyndromeSaddam ZakariyaBelum ada peringkat
- Laporan Kasus IschialgiaDokumen32 halamanLaporan Kasus Ischialgiadeviinatalia0% (1)
- Makalah Fisioterapi Pada ParkinsonDokumen14 halamanMakalah Fisioterapi Pada ParkinsonGabriela Febriadum RandaBelum ada peringkat
- Pemeriksaan IschialgiaDokumen28 halamanPemeriksaan IschialgiafaizahBelum ada peringkat
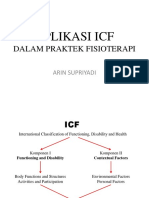
- APLIKASI ICF DLM Praktek FTDokumen30 halamanAPLIKASI ICF DLM Praktek FTDputri0% (1)
- Kelompok 1 - Lesi Pleksus Bracialis Dan LumbosakralDokumen44 halamanKelompok 1 - Lesi Pleksus Bracialis Dan LumbosakralRifa Rahmalia0% (2)
- Tes FukudaDokumen1 halamanTes FukudaakbarsepadanBelum ada peringkat
- Kelompok 5 Tennis ElbowDokumen38 halamanKelompok 5 Tennis ElbowAnnisa F. MBelum ada peringkat
- Cervical Root SyndromeDokumen34 halamanCervical Root SyndromeArief Tri YuliyantoBelum ada peringkat
- Pengukuran ROM Wrist and HandDokumen22 halamanPengukuran ROM Wrist and HandYulia M. SBelum ada peringkat
- Nyeri Gluteal Dan Paha Belakang Sacroiliac Joint Up Slipe BlockadeDokumen2 halamanNyeri Gluteal Dan Paha Belakang Sacroiliac Joint Up Slipe BlockadeAnanta MiaBelum ada peringkat
- Makalah IschialgiaDokumen22 halamanMakalah Ischialgiadwiliviasari100% (1)
- TFCCDokumen17 halamanTFCCcipa100% (1)
- BursitisDokumen18 halamanBursitisZara YunitaBelum ada peringkat
- Pemeriksaan Lutut 1Dokumen40 halamanPemeriksaan Lutut 1Rehani Pradipta100% (1)
- LBP Ec HNPDokumen25 halamanLBP Ec HNPfajarcolzzzBelum ada peringkat
- Referat Tennis ElbowDokumen33 halamanReferat Tennis ElbowbismooBelum ada peringkat
- PPT Herpes ZoosterDokumen21 halamanPPT Herpes ZoosterDini Tyas100% (1)
- Cara Melakukan Pemeriksaan Fisik BahuDokumen10 halamanCara Melakukan Pemeriksaan Fisik Bahupsari_1967% (3)
- Gun Stock Deformity-1Dokumen27 halamanGun Stock Deformity-1Chill NggataBelum ada peringkat
- Lesi MedianusDokumen15 halamanLesi MedianusSetio Dwi AtmojoBelum ada peringkat
- LBP Akibat HNPDokumen19 halamanLBP Akibat HNPnurfaidahBelum ada peringkat
- Rangkuman MR Rehab MedikDokumen21 halamanRangkuman MR Rehab MedikReviandy ArmandaniBelum ada peringkat
- Pemeriksaan Spesifik Regio VertebraDokumen18 halamanPemeriksaan Spesifik Regio VertebraAinun UrbubiyahBelum ada peringkat
- Pemeriksaan Spesifik Fisioterapi..Dokumen11 halamanPemeriksaan Spesifik Fisioterapi..Kanliajie Kresna KastiantoBelum ada peringkat
- Pemeriksaan Spesifik Anggota Gerak Atas Dan BawahDokumen25 halamanPemeriksaan Spesifik Anggota Gerak Atas Dan BawahreniBelum ada peringkat
- Spesial Test CervicalDokumen22 halamanSpesial Test CervicalBrilian DinantiBelum ada peringkat
- 5 KPDM Stress Dan Mpe - DR DeaDokumen33 halaman5 KPDM Stress Dan Mpe - DR DeawiranirwanaBelum ada peringkat
- Program Kerja Senat Siswa Dikspespa 2019 BaruDokumen7 halamanProgram Kerja Senat Siswa Dikspespa 2019 BaruwiranirwanaBelum ada peringkat
- Soal Mandiri Ukmppd 2010-1Dokumen69 halamanSoal Mandiri Ukmppd 2010-1wiranirwanaBelum ada peringkat
- Morning Report PEB TIM BDokumen17 halamanMorning Report PEB TIM BwiranirwanaBelum ada peringkat
- Responsi ADHFDokumen39 halamanResponsi ADHFwiranirwanaBelum ada peringkat
- STEMI (ST Elevation Myocardial Infarction)Dokumen25 halamanSTEMI (ST Elevation Myocardial Infarction)wiranirwanaBelum ada peringkat
- OSCE NEURO + Jawaban Meilinda TerbaruDokumen12 halamanOSCE NEURO + Jawaban Meilinda TerbaruwiranirwanaBelum ada peringkat
- Rangkuman Man Man ManDokumen14 halamanRangkuman Man Man ManwiranirwanaBelum ada peringkat
- Responsi TB + PNEUMONIA CAPDokumen67 halamanResponsi TB + PNEUMONIA CAPwiranirwanaBelum ada peringkat
- Morning Report ParuDokumen16 halamanMorning Report ParuwiranirwanaBelum ada peringkat
- Syok SepsisDokumen26 halamanSyok SepsiswiranirwanaBelum ada peringkat
- Radiologi Unibraw Catetan KoasDokumen81 halamanRadiologi Unibraw Catetan KoasAndri100% (6)
- Responsi ISK FixDokumen38 halamanResponsi ISK FixMeilinda SusiloriniBelum ada peringkat
- Responsi Anemia Defisiensi Besi DR Djoko SPPDDokumen23 halamanResponsi Anemia Defisiensi Besi DR Djoko SPPDwiranirwanaBelum ada peringkat