Anda mungkin juga menyukai
- LP Meningoensefalitis Megawati YunusDokumen43 halamanLP Meningoensefalitis Megawati YunusMhega Yunus100% (4)
- LP Meningitis Nurul Belum FixDokumen15 halamanLP Meningitis Nurul Belum FixNurul Hayati BBelum ada peringkat
- PP Refrat EnsefalitisDokumen36 halamanPP Refrat Ensefalitisdhana_494100% (2)
- Laporan Pendahuluan Pada Pasien Dengan MeningoensefalitisDokumen17 halamanLaporan Pendahuluan Pada Pasien Dengan MeningoensefalitisDewi UlfatiBelum ada peringkat
- EnchepalitisDokumen26 halamanEnchepalitisKeysha NisrinaBelum ada peringkat
- LP Meningoensefalitis FIXDokumen24 halamanLP Meningoensefalitis FIXanugrah satriaBelum ada peringkat
- Laporan Pendahuluan Meningoensefalitis ViralDokumen14 halamanLaporan Pendahuluan Meningoensefalitis ViralM. ATFHAL RAMADANABelum ada peringkat
- Laporan Pendahuluan Pada Pasien Dengan MeningoensefalitisDokumen16 halamanLaporan Pendahuluan Pada Pasien Dengan MeningoensefalitisAyu Lisna Pratiwie100% (1)
- Referat MeningitisDokumen38 halamanReferat MeningitisVini TienBelum ada peringkat
- Definisi EncephalitisDokumen17 halamanDefinisi EncephalitisPhytata HandayaniBelum ada peringkat
- Contoh Case EnsefalitisDokumen34 halamanContoh Case EnsefalitisAbqariyah TaisirBelum ada peringkat
- Referat Ensefalitis Pada AnakDokumen15 halamanReferat Ensefalitis Pada AnakAsa Russevi UtamiBelum ada peringkat
- EnsefelatisDokumen14 halamanEnsefelatisClara Mutiara EdemBelum ada peringkat
- INFEKSI (Lengkap)Dokumen137 halamanINFEKSI (Lengkap)dediunggulBelum ada peringkat
- Referat MeningitisDokumen28 halamanReferat Meningitisalvionita citraBelum ada peringkat
- Askep EncephalitisDokumen17 halamanAskep EncephalitisAnonymous mipMg0aVBelum ada peringkat
- LP Meningoenchepalitis RevisiDokumen17 halamanLP Meningoenchepalitis RevisiLutfi nrnBelum ada peringkat
- LP Meningitis AnakDokumen21 halamanLP Meningitis AnakFitri Ekaharining Tias100% (1)
- LAPORAN PENDAHULUAN MENINGITIS PADA ANAK FixDokumen18 halamanLAPORAN PENDAHULUAN MENINGITIS PADA ANAK Fixfandimuhamad.jobsBelum ada peringkat
- Radang OtakDokumen13 halamanRadang OtakKeren RivaiBelum ada peringkat
- Ensefalitis Meningitis NEWDokumen41 halamanEnsefalitis Meningitis NEWmuh hardiansyahBelum ada peringkat
- LP MeningoensefalitisDokumen12 halamanLP MeningoensefalitisFatimah ElyaniBelum ada peringkat
- Asuhan Keperawatan Encephalitis SaeDokumen18 halamanAsuhan Keperawatan Encephalitis SaeMentari AldilaBelum ada peringkat
- EncephalitisDokumen26 halamanEncephalitisFebrian Wahyu RamadhaniBelum ada peringkat
- Bab IiDokumen22 halamanBab IiAdhyaksa Indrajid KurawaBelum ada peringkat
- Tabel Perbedaan Meningitis Dan EnsefalitisDokumen7 halamanTabel Perbedaan Meningitis Dan EnsefalitisFajarPambudiBelum ada peringkat
- Laporan Pendahuluan-2Dokumen11 halamanLaporan Pendahuluan-2Say MitaBelum ada peringkat
- ENSEFALITISDokumen21 halamanENSEFALITISTira KurniatiBelum ada peringkat
- LP EnsefalitisDokumen7 halamanLP EnsefalitisArif AshariBelum ada peringkat
- EnsefalitisDokumen6 halamanEnsefalitisIcha DanisaBelum ada peringkat
- Laporan Pendahuluan Meningo EnsefalitisDokumen20 halamanLaporan Pendahuluan Meningo Ensefalitisnelpi pobelaBelum ada peringkat
- TINJAUAN PUSTAKA MeningoensefalitisDokumen8 halamanTINJAUAN PUSTAKA MeningoensefalitisariadiBelum ada peringkat
- Infeksi Sistem Saraf PusatDokumen11 halamanInfeksi Sistem Saraf Pusatami tri nursasmiBelum ada peringkat
- EnsefalitisDokumen16 halamanEnsefalitisAdinda Suci MaghfiraBelum ada peringkat
- Askep Encephalitis Kelompok 2Dokumen26 halamanAskep Encephalitis Kelompok 2Klara JuvangkaBelum ada peringkat
- Tentir K9. Mikrobiologi Neurosains PULMO'16Dokumen20 halamanTentir K9. Mikrobiologi Neurosains PULMO'16Zehrotus SholihahBelum ada peringkat
- ENSEFALITISDokumen31 halamanENSEFALITISBastian SimorangkirBelum ada peringkat
- 7 NeuroinfeksiDokumen64 halaman7 NeuroinfeksiAndiy Yaniz'sBelum ada peringkat
- Etiologi Dan Patofisiologi Infeksi Susunan Saraf PusatDokumen4 halamanEtiologi Dan Patofisiologi Infeksi Susunan Saraf Pusatmuhammad ajiBelum ada peringkat
- LP+ASKEp Meningitis MelatiDokumen53 halamanLP+ASKEp Meningitis MelatiZiadah N. Rizqiyah100% (1)
- Mikroorganisme Penyebab Infeksi Sistem Saraf FinalDokumen69 halamanMikroorganisme Penyebab Infeksi Sistem Saraf FinalAloysius Anangga HBelum ada peringkat
- EnsefalitisDokumen10 halamanEnsefalitisZulhamBelum ada peringkat
- Ensefalitis LengkapDokumen21 halamanEnsefalitis LengkapEll ZeinBelum ada peringkat
- Askep Meningitis FixDokumen55 halamanAskep Meningitis FixLilis Dwi SeptianiBelum ada peringkat
- Presentasi Referat - Infeksi SSP - Maria Ducis Nurak BanunaekDokumen34 halamanPresentasi Referat - Infeksi SSP - Maria Ducis Nurak BanunaekChyndi dami 1216Belum ada peringkat
- LP Encephalitis HanihDokumen19 halamanLP Encephalitis HanihMyoui minaBelum ada peringkat
- LP MeningitisDokumen15 halamanLP Meningitisnorma zeeBelum ada peringkat
- EnsefalitisDokumen10 halamanEnsefalitisCynthiaRimbaBelum ada peringkat
- Makalah EnchepalitisDokumen20 halamanMakalah Enchepalitisarumingtyas pawestriBelum ada peringkat
- LAPORAN PENDAHULUAN ASUHAN KEPERAWATAN PADA PASIEN DENGAN ENCEPHALITIS DI RUANG KASWARI RUMAH SAKIT UMUM DAERAH WANGAYA-dikonversiDokumen13 halamanLAPORAN PENDAHULUAN ASUHAN KEPERAWATAN PADA PASIEN DENGAN ENCEPHALITIS DI RUANG KASWARI RUMAH SAKIT UMUM DAERAH WANGAYA-dikonversiWiwi 1998Belum ada peringkat
- Andra Yuliandi - CRS Meningitis TBDokumen31 halamanAndra Yuliandi - CRS Meningitis TBpoppyBelum ada peringkat
- Ensefalitis - Winda Fahiratunnisa.Dokumen21 halamanEnsefalitis - Winda Fahiratunnisa.Winda FRBelum ada peringkat
- Referat Meningitis VirusDokumen28 halamanReferat Meningitis VirusMatthew Kevin HendriantoBelum ada peringkat
- ENSEFALITISDokumen19 halamanENSEFALITISteduhBelum ada peringkat
- Meningitis AnakDokumen26 halamanMeningitis AnakGracitaGeminicaBelum ada peringkat
- MeningoencephalitisDokumen57 halamanMeningoencephalitisNijimura Shuuzo100% (1)
- LAPORAN PENDAHULUAN ASUHAN KEPERAWATAN PADA PASIEN DENGAN ENCEPHALITIS DI RUANG KASWARI RUMAH SAKIT UMUM DAERAH WANGAYA-dikonversiDokumen13 halamanLAPORAN PENDAHULUAN ASUHAN KEPERAWATAN PADA PASIEN DENGAN ENCEPHALITIS DI RUANG KASWARI RUMAH SAKIT UMUM DAERAH WANGAYA-dikonversiWiwi 1998Belum ada peringkat
- Mikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaDari EverandMikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaPenilaian: 2.5 dari 5 bintang2.5/5 (2)
- Mikrobiologi Medis I: Patogen dan Mikrobioma ManusiaDari EverandMikrobiologi Medis I: Patogen dan Mikrobioma ManusiaPenilaian: 4 dari 5 bintang4/5 (11)
- Coronavirus Covid-19. Membela diri. Cara menghindari penularan. Bagaimana melindungi keluarga dan pekerjaan Anda. Diperbarui edisi keempat.Dari EverandCoronavirus Covid-19. Membela diri. Cara menghindari penularan. Bagaimana melindungi keluarga dan pekerjaan Anda. Diperbarui edisi keempat.Penilaian: 5 dari 5 bintang5/5 (2)
- Kelompok B BST Skabies Dr. Rahmila Sari Sp. DVDokumen32 halamanKelompok B BST Skabies Dr. Rahmila Sari Sp. DVZhafran TobingBelum ada peringkat
- Kelompok B BST Scabies - Dr. RirinDokumen13 halamanKelompok B BST Scabies - Dr. RirinZhafran TobingBelum ada peringkat
- Referat Kelompok B PiodermaDokumen36 halamanReferat Kelompok B PiodermaZhafran TobingBelum ada peringkat
- RK Kelompok B Impetigo Krustosa Dr. Dina SP - DVDokumen29 halamanRK Kelompok B Impetigo Krustosa Dr. Dina SP - DVZhafran TobingBelum ada peringkat
- Case ReportDokumen12 halamanCase ReportZhafran TobingBelum ada peringkat
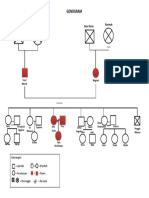
- GenogramDokumen1 halamanGenogramZhafran TobingBelum ada peringkat
- Buku Panduan CSL 1 2015Dokumen134 halamanBuku Panduan CSL 1 2015Zhafran TobingBelum ada peringkat
- Family Assessment ZhafranDokumen8 halamanFamily Assessment ZhafranZhafran TobingBelum ada peringkat
- Antropologi Medis Dr. TALDokumen14 halamanAntropologi Medis Dr. TALZhafran TobingBelum ada peringkat
- Batuk Darah Dr. NinaDokumen37 halamanBatuk Darah Dr. NinaZhafran TobingBelum ada peringkat
- GONIOMETRI Dr. SanjotoDokumen4 halamanGONIOMETRI Dr. SanjotoZhafran TobingBelum ada peringkat
- Diet Pada Gangguan Kesehatan Jiwa Dr. DianDokumen14 halamanDiet Pada Gangguan Kesehatan Jiwa Dr. DianZhafran TobingBelum ada peringkat
- Agromedicine Definisi Dan Ruang Lingkup Dr. DianaDokumen15 halamanAgromedicine Definisi Dan Ruang Lingkup Dr. DianaZhafran TobingBelum ada peringkat
- Sirkulus WillisiDokumen10 halamanSirkulus WillisiZhafran TobingBelum ada peringkat
- Materi Medical Emergency Response Plan BasarnasDokumen32 halamanMateri Medical Emergency Response Plan BasarnasZhafran TobingBelum ada peringkat