Anda mungkin juga menyukai
- Profil Farmakologi Obat Anti Viral Hepatitis B KronikDokumen10 halamanProfil Farmakologi Obat Anti Viral Hepatitis B KronikPebriana0% (1)
- Kelompok 4 Hepatitis BDokumen33 halamanKelompok 4 Hepatitis BLyna AmaliaBelum ada peringkat
- Obat Pada Sistem HepatobilierDokumen46 halamanObat Pada Sistem HepatobilierWiwin WinartiBelum ada peringkat
- Tatalaksana Hep B KronikDokumen3 halamanTatalaksana Hep B Kronikdysha hasyaBelum ada peringkat
- Makalah Konsep Dasar DAN Askep Hepatitis - A. Latar Belakang Penyakit Hepatitis, Lazim Dikenal - StudocuDokumen3 halamanMakalah Konsep Dasar DAN Askep Hepatitis - A. Latar Belakang Penyakit Hepatitis, Lazim Dikenal - Studocumelisaa swaraaBelum ada peringkat
- Referat Hepatitis BDokumen10 halamanReferat Hepatitis BAxel NikeBelum ada peringkat
- Hepatitis BDokumen17 halamanHepatitis BRaja Friska YulandaBelum ada peringkat
- Kelompok 5 HepatititsDokumen18 halamanKelompok 5 HepatititsEka ZulaikaBelum ada peringkat
- Penatalaksanaan Hepatitis BDokumen13 halamanPenatalaksanaan Hepatitis BSherly Rorong0% (1)
- REFERAT Besar PPT FixDokumen48 halamanREFERAT Besar PPT FixRahayu Sri WahyuniBelum ada peringkat
- Kelompok 5-HepatitisDokumen44 halamanKelompok 5-HepatitisGrey Matter DcrBelum ada peringkat
- PengobatanDokumen6 halamanPengobatannataliaBelum ada peringkat
- Penatalaksaan HepatitisDokumen5 halamanPenatalaksaan HepatitisSylvia Nur KartikaBelum ada peringkat
- PRS Bu Vita - KASUS 2 HEPATITIS B - KEL.2 (A4)Dokumen37 halamanPRS Bu Vita - KASUS 2 HEPATITIS B - KEL.2 (A4)diana nur aulia sariBelum ada peringkat
- PRS Bu Vita - KASUS 2 HEPATITIS B - KEL.2 (A4)Dokumen36 halamanPRS Bu Vita - KASUS 2 HEPATITIS B - KEL.2 (A4)diana nur aulia sariBelum ada peringkat
- Hepatitis B KronikDokumen8 halamanHepatitis B KronikVianney LiBelum ada peringkat
- Terapi Interveron HCVDokumen20 halamanTerapi Interveron HCVdonkeyendutBelum ada peringkat
- Jurnal Terapi Hepatitis CDokumen16 halamanJurnal Terapi Hepatitis CESHA FAHLUTHFIBelum ada peringkat
- EntecavirDokumen3 halamanEntecavirIntan PermatasariBelum ada peringkat
- Kelompok 2 (Hepatitis) Farmakoterapi UASDokumen37 halamanKelompok 2 (Hepatitis) Farmakoterapi UASawalia muna lorensaBelum ada peringkat
- 7Dokumen3 halaman7Ah AhBelum ada peringkat
- Tutorial Mata KuningDokumen5 halamanTutorial Mata KuningIda bagus Sathya dharma nandaBelum ada peringkat
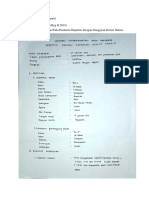
- Tugas-8 Askep Penderita Hepatitis Dengan Gangguan Defisit Nutrisi-04021281924104-Nabila Ariyani Saputri-Reg B 2019Dokumen14 halamanTugas-8 Askep Penderita Hepatitis Dengan Gangguan Defisit Nutrisi-04021281924104-Nabila Ariyani Saputri-Reg B 2019nabilaBelum ada peringkat
- REFERAT Hepatitis BDokumen32 halamanREFERAT Hepatitis BAthena S FauziaBelum ada peringkat
- Penatalaksanaan HepatitisDokumen15 halamanPenatalaksanaan HepatitisDianAndikaBelum ada peringkat
- Gangguan Hati Dan Batu Empedu FixDokumen77 halamanGangguan Hati Dan Batu Empedu FixTiya SafariniBelum ada peringkat
- Manifestasi KlinisDokumen6 halamanManifestasi KlinisNindiTyaraBelum ada peringkat
- Koinfeksi HIVDokumen56 halamanKoinfeksi HIVNanda MaisyuriBelum ada peringkat
- Hepatitis BDokumen7 halamanHepatitis Bzuhri090Belum ada peringkat
- Kelompok3 Liver&HepatitisDokumen22 halamanKelompok3 Liver&HepatitisANNISA FAJRINBelum ada peringkat
- Farter 3 - HepatitisDokumen59 halamanFarter 3 - HepatitisAjeng AfrilianaBelum ada peringkat
- Hepatitis A, BDokumen36 halamanHepatitis A, BYeny ElfiyantiBelum ada peringkat
- Laporan 1 Pencegahan Infeksi Hepatitis BDokumen10 halamanLaporan 1 Pencegahan Infeksi Hepatitis BSeftiaini NurifatimahBelum ada peringkat
- B6 - Case Hepatitis - Farmakoterapi 2Dokumen3 halamanB6 - Case Hepatitis - Farmakoterapi 2ibnu an nafisBelum ada peringkat
- Antivirus Untuk HBV Dan HCVDokumen5 halamanAntivirus Untuk HBV Dan HCVribnu31Belum ada peringkat
- HEPATITISDokumen68 halamanHEPATITISDanyx Reistanza100% (2)
- K-4 Kasus HatiDokumen31 halamanK-4 Kasus HatiCitra AmaliaBelum ada peringkat
- Kasus Gangguan Hati, Kelompok 4Dokumen30 halamanKasus Gangguan Hati, Kelompok 4Ira faziraBelum ada peringkat
- 2.2.1. PencegahanDokumen3 halaman2.2.1. PencegahanAh AhBelum ada peringkat
- Hepatitis B KronikDokumen61 halamanHepatitis B KronikTinawulaa AswadBelum ada peringkat
- Journal Obgyn FixDokumen33 halamanJournal Obgyn FixLina UkagoBelum ada peringkat
- Askep Hepatitis (Studos)Dokumen21 halamanAskep Hepatitis (Studos)Ulfa Solfadilla100% (1)
- (Eri Dan Mita) Penatalaksanaan HepatitisDokumen4 halaman(Eri Dan Mita) Penatalaksanaan HepatitisVirna SoaresBelum ada peringkat
- Tinjauan Pustaka Hepatitis B KronikDokumen8 halamanTinjauan Pustaka Hepatitis B KronikKhoirunnisa Qurrota'ayun Nur UtamiBelum ada peringkat
- Hepatitis Dan SirosisDokumen11 halamanHepatitis Dan SirosisRaina96Belum ada peringkat
- Entecavir: A Potent New Antiviral Drug For Hepatitis BDokumen7 halamanEntecavir: A Potent New Antiviral Drug For Hepatitis BILaaBelum ada peringkat
- Worksheet Hepatitis B FixDokumen6 halamanWorksheet Hepatitis B FixDhe Herdy RiliansahBelum ada peringkat
- Farmakoterapi Hepatitis: Dr. William, SP - FK Departemen Farmakologi FKIK UKRIDADokumen57 halamanFarmakoterapi Hepatitis: Dr. William, SP - FK Departemen Farmakologi FKIK UKRIDAEstinovayantiBelum ada peringkat
- Patogenesis Hepatitis A Rana DRDokumen7 halamanPatogenesis Hepatitis A Rana DRMahesa SuryanagaraBelum ada peringkat
- Hepatitis BDokumen33 halamanHepatitis BAdistha TofanoBelum ada peringkat
- Farmakologi Dan Terapi HepatitisDokumen51 halamanFarmakologi Dan Terapi HepatitisTRI CAHYANI100% (3)
- Kelompok IPDVDokumen24 halamanKelompok IPDVDindaGaluhPitalokaBelum ada peringkat
- Askep HepatitisDokumen28 halamanAskep HepatitisLutfiatulaksmi Gaen FarlinaBelum ada peringkat
- Pemeriksaan Penunjang HepatitisDokumen3 halamanPemeriksaan Penunjang HepatitisVithaBelum ada peringkat
- Product Insert EntecavirDokumen6 halamanProduct Insert EntecavirArridhoBelum ada peringkat
- Penatalaksanaan Hepatitis 1Dokumen10 halamanPenatalaksanaan Hepatitis 1Ayu MustikariniBelum ada peringkat
- Pedoman HepatitisDokumen5 halamanPedoman HepatitismeutiaputripuyBelum ada peringkat
- Tumbuhan Herbal Yang Berkhasiat Mencegah Wabah Penyakit Edisi Bahasa Inggris 2021Dari EverandTumbuhan Herbal Yang Berkhasiat Mencegah Wabah Penyakit Edisi Bahasa Inggris 2021Belum ada peringkat
- Mikrobiologi Medis I: Patogen dan Mikrobioma ManusiaDari EverandMikrobiologi Medis I: Patogen dan Mikrobioma ManusiaPenilaian: 4 dari 5 bintang4/5 (11)
- Mikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaDari EverandMikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaPenilaian: 2.5 dari 5 bintang2.5/5 (2)