Anda mungkin juga menyukai
- Hematologi KlinikDokumen22 halamanHematologi Klinikmichaelsophian100% (1)
- SOAL_HOMDokumen35 halamanSOAL_HOMric_vir_014Belum ada peringkat
- Soal Kasus Hematologi III (Polisitemia) Juwy Trianes PDFDokumen1 halamanSoal Kasus Hematologi III (Polisitemia) Juwy Trianes PDFjuwy trianesBelum ada peringkat
- KASUS SOAL KELOMPOK 3Dokumen4 halamanKASUS SOAL KELOMPOK 3syafir50% (2)
- Kimia KlinikDokumen40 halamanKimia KlinikEndah NovprianiBelum ada peringkat
- TOKSIKOLOGIDokumen24 halamanTOKSIKOLOGIRasmahhBelum ada peringkat
- Soal HematologiDokumen23 halamanSoal HematologiNur Asy SyamsiBelum ada peringkat
- soal TD komponen darahDokumen11 halamansoal TD komponen darahnadhilah hani pBelum ada peringkat
- Soal Sirosis HepatisDokumen6 halamanSoal Sirosis HepatisHilda Aprilia Pratiwi0% (1)
- Soal Soal LEUKEMIA KRONISDokumen9 halamanSoal Soal LEUKEMIA KRONIScitraBelum ada peringkat
- SOAL UJIAN IMUNOLOGIDokumen1 halamanSOAL UJIAN IMUNOLOGIBayu ChrispriantiBelum ada peringkat
- Soal Bilirubin Indirek PRAKTEK, Kelompok 7Dokumen3 halamanSoal Bilirubin Indirek PRAKTEK, Kelompok 7Aji RahmanBelum ada peringkat
- Soal Demam Tifoid Kel IVDokumen2 halamanSoal Demam Tifoid Kel IVMareta AkhriansyahBelum ada peringkat
- ToksikologiDokumen9 halamanToksikologiJ JKBelum ada peringkat
- Latihan SoalDokumen15 halamanLatihan SoalUlfahBelum ada peringkat
- Soal Soal Hepatitis A Dan BDokumen3 halamanSoal Soal Hepatitis A Dan BDisco_smucamBelum ada peringkat
- Infeksi HatiDokumen2 halamanInfeksi HatiNurAlfhyahZahrahBelum ada peringkat
- Kumpulan Tugas Membuat Soal Pilihan Ganda HematologiDokumen17 halamanKumpulan Tugas Membuat Soal Pilihan Ganda HematologiMutiahAchmad 2019Belum ada peringkat
- Soal LeukimiaDokumen4 halamanSoal LeukimiaSri Rahayu KadirBelum ada peringkat
- PK LEUKEMIADokumen4 halamanPK LEUKEMIAAnita Dwi Rachmawati100% (2)
- Soal Imunoserologi PPSDMDokumen8 halamanSoal Imunoserologi PPSDMAisyah HakimBelum ada peringkat
- Kumpulan Soal Kep KritisDokumen14 halamanKumpulan Soal Kep KritisLiance100% (1)
- Kandidiasis BayiDokumen30 halamanKandidiasis BayiDhimasAjiZuandaBelum ada peringkat
- Contoh SoalDokumen2 halamanContoh Soalcitra_hidayatBelum ada peringkat
- Soal Pilihan Ganda Kimia Klinik Dan DiagnostiDokumen7 halamanSoal Pilihan Ganda Kimia Klinik Dan DiagnostiYatil HidayaniBelum ada peringkat
- Blok 10 SoalDokumen13 halamanBlok 10 SoalKornelis Aribowo100% (2)
- TO Ukom 2 Hematologi-1Dokumen6 halamanTO Ukom 2 Hematologi-1Novi NurhidayahBelum ada peringkat
- 012 - Delianti - Soal Kasus Toksikologi KlinikDokumen2 halaman012 - Delianti - Soal Kasus Toksikologi KlinikMuhammad RaihandBelum ada peringkat
- OPTIMASI FAAL HATIDokumen27 halamanOPTIMASI FAAL HATIAfika AuliaBelum ada peringkat
- SOAL KMB LeukemiaDokumen1 halamanSOAL KMB LeukemiaUtinBelum ada peringkat
- Bank Soal Anemia Dan Transfusi DarahDokumen23 halamanBank Soal Anemia Dan Transfusi DarahDinan Bagja NugrahaBelum ada peringkat
- Soal Latihan Responsi Mikrobiologi Blok UrogenitalDokumen5 halamanSoal Latihan Responsi Mikrobiologi Blok UrogenitalGrace Kalpika Taruli SiagianBelum ada peringkat
- Soal HipotiroidDokumen9 halamanSoal HipotiroidMey hulopiBelum ada peringkat
- Soal Leukemia AnakDokumen3 halamanSoal Leukemia AnakAhaddin YusufBelum ada peringkat
- Kelompok 1Dokumen23 halamanKelompok 1Aisyah Aviva100% (1)
- PertanyaanDokumen5 halamanPertanyaanDeniDianaBelum ada peringkat
- Pemeriksaan Laboratorium untuk Diagnosis Penyakit pada HewanDokumen6 halamanPemeriksaan Laboratorium untuk Diagnosis Penyakit pada HewanRyne BalweelBelum ada peringkat
- Difteri SoalDokumen2 halamanDifteri SoalTjoema AsriBelum ada peringkat
- Soal KMB Kelompok 18 ThalasemiaDokumen6 halamanSoal KMB Kelompok 18 ThalasemiaJoko RifaiBelum ada peringkat
- Soal Leukimia MCQDokumen2 halamanSoal Leukimia MCQRiadinniAlitaBelum ada peringkat
- Soal Dan Jawaban System ImunitasDokumen10 halamanSoal Dan Jawaban System ImunitasrinaBelum ada peringkat
- Soal ImunDokumen4 halamanSoal ImunRif'ah SabariahBelum ada peringkat
- JUDULDokumen24 halamanJUDULSiti MariamBelum ada peringkat
- Kasus 1 Soal No.2 Patfis LabDokumen12 halamanKasus 1 Soal No.2 Patfis LabIcha NathaliaBelum ada peringkat
- Soal Autoimun DiseaseDokumen2 halamanSoal Autoimun DiseaseAlief Abni Bernindra100% (1)
- Hematologi Manual DasarDokumen223 halamanHematologi Manual Dasarshanti ayuBelum ada peringkat
- Penyakit Hisprung Pada AnakDokumen25 halamanPenyakit Hisprung Pada AnakAsmita Cahya AzisBelum ada peringkat
- PEMERIKSAAN ELEKTROLIT DARAHDokumen54 halamanPEMERIKSAAN ELEKTROLIT DARAHWidya NingrumBelum ada peringkat
- Soal ImmunoserologiDokumen7 halamanSoal ImmunoserologiAndi UkengBelum ada peringkat
- PertusisDokumen3 halamanPertusisMuhammad Fauzan FebrianBelum ada peringkat
- Pemeriksaan LaboratoriumDokumen5 halamanPemeriksaan LaboratoriummuchanakbaeBelum ada peringkat
- SOAL KASUS ANAK 3 THALASEMIA Dan Kelainan Kongenital Kel.5Dokumen3 halamanSOAL KASUS ANAK 3 THALASEMIA Dan Kelainan Kongenital Kel.5Yana TalapessyBelum ada peringkat
- KULTUR JARINGANDokumen28 halamanKULTUR JARINGANPurnama EkasariBelum ada peringkat
- 115 Soal Parasitologi (Edit)Dokumen29 halaman115 Soal Parasitologi (Edit)IndahBelum ada peringkat
- PEMERIKSAAN HEMATOLOGIDokumen16 halamanPEMERIKSAAN HEMATOLOGIsiti rodiyahBelum ada peringkat
- PilihanGandaMikrobiologiDokumen7 halamanPilihanGandaMikrobiologiRonny SagulaniBelum ada peringkat
- HEMATOPOIESISDokumen57 halamanHEMATOPOIESISFrengky RiyantoBelum ada peringkat
- MCQ 5.2 Tentang Hematologi dan Transfusi DarahDokumen21 halamanMCQ 5.2 Tentang Hematologi dan Transfusi DarahEfanPutraBelum ada peringkat
- Fix Tojeng TojengDokumen19 halamanFix Tojeng TojengBaso Nuzul MaqfirBelum ada peringkat
- Soal Uts Farmakoterapi 3 Untuk RegularDokumen14 halamanSoal Uts Farmakoterapi 3 Untuk Regularmega aryantiBelum ada peringkat
- Ringkasan Komunikasi Terapeutik Pertemuan 1 - Poppy Ayu Namira - 1711011040 - Kelas BDokumen3 halamanRingkasan Komunikasi Terapeutik Pertemuan 1 - Poppy Ayu Namira - 1711011040 - Kelas BPoppyA.NamiraBelum ada peringkat
- EpilepsiDokumen6 halamanEpilepsiPoppyA.NamiraBelum ada peringkat
- Meningitis terapi farmakologiDokumen3 halamanMeningitis terapi farmakologiPoppyA.NamiraBelum ada peringkat
- Kasus 5 - Farmakoterapi TonsilitisDokumen1 halamanKasus 5 - Farmakoterapi TonsilitisPoppyA.NamiraBelum ada peringkat
- Resume Dan Soal FE MCQ Pertemuan 3Dokumen5 halamanResume Dan Soal FE MCQ Pertemuan 3PoppyA.NamiraBelum ada peringkat
- Poppy Ayu Namira - 1711011040 - Resume Stem CellDokumen15 halamanPoppy Ayu Namira - 1711011040 - Resume Stem CellPoppyA.NamiraBelum ada peringkat
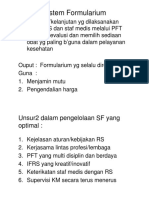
- Sistem Formularium PDFDokumen13 halamanSistem Formularium PDFPoppyA.NamiraBelum ada peringkat
- Sistem Formularium PDFDokumen13 halamanSistem Formularium PDFPoppyA.NamiraBelum ada peringkat
- Epilepsi Dian Ayu 2020 PDFDokumen38 halamanEpilepsi Dian Ayu 2020 PDFPoppyA.NamiraBelum ada peringkat
- Lanjutan Diagnosa Dan Staging, Terapi Kanker (Operasi, Radiasi, Kemoterapi, Hormon Terapi Dan Biologi Terapi) (Topik 4) PDFDokumen37 halamanLanjutan Diagnosa Dan Staging, Terapi Kanker (Operasi, Radiasi, Kemoterapi, Hormon Terapi Dan Biologi Terapi) (Topik 4) PDFPoppyA.NamiraBelum ada peringkat
- Poppy Ayu Namira - 1711011040 - Resume Jurnal DismenoreaDokumen7 halamanPoppy Ayu Namira - 1711011040 - Resume Jurnal DismenoreaPoppyA.NamiraBelum ada peringkat
- Praktikum Tablet (3-30-2020)Dokumen9 halamanPraktikum Tablet (3-30-2020)PoppyA.NamiraBelum ada peringkat
- Poppy Ayu Namira - 1711011040 - L1 PDFDokumen2 halamanPoppy Ayu Namira - 1711011040 - L1 PDFPoppyA.NamiraBelum ada peringkat
- B1 - Poppy Ayu Namira - 1711011040 PDFDokumen1 halamanB1 - Poppy Ayu Namira - 1711011040 PDFPoppyA.NamiraBelum ada peringkat
- Tugas Bu Henny TaniaDokumen2 halamanTugas Bu Henny TaniaPoppyA.NamiraBelum ada peringkat
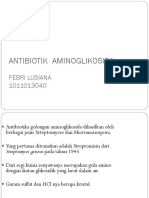
- Antibiotik AminoglikosidaDokumen28 halamanAntibiotik AminoglikosidaRarys 18Belum ada peringkat
- Mengenal Siklus Sel, Proses Kematian Sel, Diagnosa Dan Tumor Staging (Topik 3) PDFDokumen27 halamanMengenal Siklus Sel, Proses Kematian Sel, Diagnosa Dan Tumor Staging (Topik 3) PDFPoppyA.NamiraBelum ada peringkat
- Ekskresi Obat BFDokumen20 halamanEkskresi Obat BFPoppyA.NamiraBelum ada peringkat
- Multiple Choice For Uas ft3-2018Dokumen5 halamanMultiple Choice For Uas ft3-2018PoppyA.NamiraBelum ada peringkat
- BUD OBAT RACIKANDokumen18 halamanBUD OBAT RACIKANPoppyA.NamiraBelum ada peringkat
- Kel 4 IPC FIXDokumen16 halamanKel 4 IPC FIXPoppyA.NamiraBelum ada peringkat
- Kel 4 IPC FIXDokumen16 halamanKel 4 IPC FIXPoppyA.NamiraBelum ada peringkat
- Tugas Kasus BFDokumen38 halamanTugas Kasus BFPoppyA.NamiraBelum ada peringkat
- RPS Farmakoterapi I 2016 PDFDokumen17 halamanRPS Farmakoterapi I 2016 PDFagusBelum ada peringkat
- Tugas SaktiDokumen9 halamanTugas SaktiPoppyA.NamiraBelum ada peringkat
- Ocular Dosage FormDokumen25 halamanOcular Dosage FormPoppyA.NamiraBelum ada peringkat
- Bagian Mike Dan Eed (Objek 4 - HB)Dokumen3 halamanBagian Mike Dan Eed (Objek 4 - HB)PoppyA.NamiraBelum ada peringkat
- Daftar No Username Fakultas FarmasiDokumen12 halamanDaftar No Username Fakultas FarmasiPoppyA.NamiraBelum ada peringkat
- File KotakDokumen1 halamanFile KotakPoppyA.NamiraBelum ada peringkat