Anda mungkin juga menyukai
- Mikrobiologi Infeksi Jamur SistemikDokumen28 halamanMikrobiologi Infeksi Jamur SistemikPutri Nahrisyah100% (1)
- Meningitis KriptokokusDokumen37 halamanMeningitis KriptokokusCokorda Istri Dyah SintaraniBelum ada peringkat
- Infeksi Jamur Sistemik Dan Jamur OpportunisDokumen35 halamanInfeksi Jamur Sistemik Dan Jamur OpportunisIrfanBelum ada peringkat
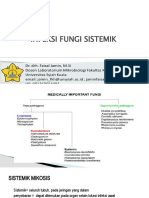
- Infeksi Jamur SistemikDokumen79 halamanInfeksi Jamur SistemikTasya FakhiraBelum ada peringkat
- Cryptococcus NeoformansDokumen4 halamanCryptococcus NeoformansnuniatmandaBelum ada peringkat
- Mikologi KlinikDokumen33 halamanMikologi KlinikST HadijahBelum ada peringkat
- Criptococcus NeofarmansDokumen21 halamanCriptococcus Neofarmansandi zsazsaBelum ada peringkat
- Mikosis OportunistikDokumen13 halamanMikosis OportunistikJum'atil Fajar100% (2)
- KELOMPOK 6 - Cryptococcus NeofarmansDokumen14 halamanKELOMPOK 6 - Cryptococcus NeofarmansMuhammad RaihandBelum ada peringkat
- Penyakit Infeksi BakteriDokumen33 halamanPenyakit Infeksi BakterimBelum ada peringkat
- Jamur ParuDokumen25 halamanJamur Paruyoan utami putriBelum ada peringkat
- Mikrobiologi JamurDokumen52 halamanMikrobiologi JamurKamilatun NiamahBelum ada peringkat
- Infeksi Jamur SistemikDokumen24 halamanInfeksi Jamur SistemikoliviamonicadBelum ada peringkat
- Infeksi Bakteri Pada Sistem KardiovaskulerDokumen33 halamanInfeksi Bakteri Pada Sistem KardiovaskulerAry MfBelum ada peringkat
- Infeksi Profunda JuniDokumen8 halamanInfeksi Profunda Junioctaviani susantiBelum ada peringkat
- Mikosis SistemikDokumen47 halamanMikosis SistemikAluihichi OkyBelum ada peringkat
- Mikosis SistemikDokumen52 halamanMikosis SistemikAisyah HakimBelum ada peringkat
- KandidiasisDokumen38 halamanKandidiasisLena PatelBelum ada peringkat
- Infeksi Jamur Saluran NafasDokumen49 halamanInfeksi Jamur Saluran NafasAthifah amaliaBelum ada peringkat
- KRIPTOKOKOSISDokumen26 halamanKRIPTOKOKOSISElly Muliati AningsihBelum ada peringkat
- Asuhan Keperawatan Anak Dengan KandidiasisDokumen19 halamanAsuhan Keperawatan Anak Dengan KandidiasisNur Amalina RahmanBelum ada peringkat
- Mikosis ProfundaDokumen74 halamanMikosis ProfundaNadiah AlbatatiBelum ada peringkat
- Mikosis Oportunistik Yang Lain Kelompo 10 MikroDokumen26 halamanMikosis Oportunistik Yang Lain Kelompo 10 MikroMarscha MaryuanaBelum ada peringkat
- Part 1 Pembahasan Seminar Optima Mei 2019 PDFDokumen1.034 halamanPart 1 Pembahasan Seminar Optima Mei 2019 PDFIrma KurniawatiBelum ada peringkat
- Dermatosis Vesikobulosa KronikDokumen45 halamanDermatosis Vesikobulosa KronikDian RianiBelum ada peringkat
- Referat SporotrikosisDokumen25 halamanReferat SporotrikosisMarwi VinaBelum ada peringkat
- PPCRYPTOSPORIDIOSISDokumen38 halamanPPCRYPTOSPORIDIOSISKresna Denta ElygioBelum ada peringkat
- Kuliah Pneumonia Blok 2.2 2020Dokumen69 halamanKuliah Pneumonia Blok 2.2 2020chicy morfiBelum ada peringkat
- 3.mikosis Oportunistik LainnyaDokumen37 halaman3.mikosis Oportunistik LainnyaNajdah HidayahBelum ada peringkat
- YeastsDokumen9 halamanYeastsJum'atil FajarBelum ada peringkat
- KANDIDIASISDokumen8 halamanKANDIDIASISAnggana Faza NazharaBelum ada peringkat
- Referat Mikosis ParuDokumen17 halamanReferat Mikosis ParuAnggina DiksitaBelum ada peringkat
- Modul Praktikum Mikrobiologi Blok Keluhan Terkait Sistem Sensoris Dan Integumentum Edisi Revisi 2023Dokumen58 halamanModul Praktikum Mikrobiologi Blok Keluhan Terkait Sistem Sensoris Dan Integumentum Edisi Revisi 2023evelynseaaBelum ada peringkat
- LTM 3 - Infeksi Oportunistik Jamur Pada Pasien Infeksi HIVDokumen7 halamanLTM 3 - Infeksi Oportunistik Jamur Pada Pasien Infeksi HIVFredy Rodeardo MaringgaBelum ada peringkat
- KRIPTOKOKOSISDokumen14 halamanKRIPTOKOKOSISNanda Nabilah UbayBelum ada peringkat
- MycoplasmosisDokumen10 halamanMycoplasmosisArief GumilarBelum ada peringkat
- LP CampakDokumen14 halamanLP CampakDwii ApriliyaniiBelum ada peringkat
- Zigomikosis 2Dokumen13 halamanZigomikosis 2Rachmad DharmawanBelum ada peringkat
- Anti JamurDokumen31 halamanAnti JamurUnhaz FkBelum ada peringkat
- Mikosis ParuDokumen56 halamanMikosis ParuBella mustika AlamBelum ada peringkat
- Deep MycosisDokumen48 halamanDeep MycosisUrinaria Kel 6Belum ada peringkat
- Bahan CandidiasisDokumen27 halamanBahan CandidiasisrivannyBelum ada peringkat
- PiodermaDokumen49 halamanPiodermaraja hackBelum ada peringkat
- FHBJDokumen10 halamanFHBJAnita PrastiwiBelum ada peringkat
- Dokumen - Tips Jamur-OportunistikDokumen21 halamanDokumen - Tips Jamur-OportunistikAjenkBelum ada peringkat
- Mikosis SistemikDokumen9 halamanMikosis SistemikAbdi Nusa Persada NababanBelum ada peringkat
- Case Report KandidiasisDokumen15 halamanCase Report Kandidiasisbeside 01Belum ada peringkat
- BBS2 MB-K10-Pyogenic Cocci Gram NegatifDokumen33 halamanBBS2 MB-K10-Pyogenic Cocci Gram NegatifThoriq Ilvan SinuratBelum ada peringkat
- Infeksi Kulit Dan Jaringan LunakDokumen21 halamanInfeksi Kulit Dan Jaringan LunakMustika Sari HutabaratBelum ada peringkat
- Konsep Mikologi 2023Dokumen36 halamanKonsep Mikologi 2023Reny RakhmawatiBelum ada peringkat
- Jamur Penyebab Infeksi Sistem Respirasi - Dr. Lisa-2Dokumen51 halamanJamur Penyebab Infeksi Sistem Respirasi - Dr. Lisa-2MilikPremiumstock90Belum ada peringkat
- Karbunkel Revisi IIDokumen12 halamanKarbunkel Revisi IIMohammad AdriansyahBelum ada peringkat
- Emergency in Dental Practice - Haryadi MangkutoDokumen20 halamanEmergency in Dental Practice - Haryadi MangkutoSaadah KurniawatiBelum ada peringkat
- Kandidiasis KutisDokumen14 halamanKandidiasis KutisBayu Jimmy SulivanBelum ada peringkat
- Clinical ReasoningDokumen25 halamanClinical ReasoningFirman FirdausBelum ada peringkat
- Mikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaDari EverandMikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaPenilaian: 2.5 dari 5 bintang2.5/5 (2)
- Mikrobiologi Medis I: Patogen dan Mikrobioma ManusiaDari EverandMikrobiologi Medis I: Patogen dan Mikrobioma ManusiaPenilaian: 4 dari 5 bintang4/5 (11)