0% menganggap dokumen ini bermanfaat (0 suara)
586 tayangan2 halamanFormulir Klaim RJ (NEW)
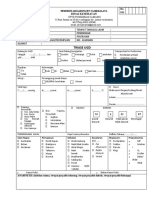
Formulir ini harus diisi untuk mengajukan klaim rawat jalan. Berisi data pasien, data medis seperti diagnosa dokter, terapi yang diterima, dan tanda tangan dokter untuk memverifikasi perawatan. Formulir ini memberi izin kepada perusahaan asuransi untuk memeriksa catatan medis terkait klaim rawat jalan pasien.
Diunggah oleh
Agust muharyadi saputroHak Cipta
© © All Rights Reserved
Kami menangani hak cipta konten dengan serius. Jika Anda merasa konten ini milik Anda, ajukan klaim di sini.
Format Tersedia
Unduh sebagai PDF, TXT atau baca online di Scribd
0% menganggap dokumen ini bermanfaat (0 suara)
586 tayangan2 halamanFormulir Klaim RJ (NEW)
Formulir ini harus diisi untuk mengajukan klaim rawat jalan. Berisi data pasien, data medis seperti diagnosa dokter, terapi yang diterima, dan tanda tangan dokter untuk memverifikasi perawatan. Formulir ini memberi izin kepada perusahaan asuransi untuk memeriksa catatan medis terkait klaim rawat jalan pasien.
Diunggah oleh
Agust muharyadi saputroHak Cipta
© © All Rights Reserved
Kami menangani hak cipta konten dengan serius. Jika Anda merasa konten ini milik Anda, ajukan klaim di sini.
Format Tersedia
Unduh sebagai PDF, TXT atau baca online di Scribd