Anda mungkin juga menyukai
- Pelaporan Insiden Keselamatan PasienDokumen38 halamanPelaporan Insiden Keselamatan PasienRetno Dhiyan PBelum ada peringkat
- Fmea KarsDokumen54 halamanFmea KarsJoe ThesecondmonthBelum ada peringkat
- Tingkat ResikoDokumen27 halamanTingkat ResikoIndra betaBelum ada peringkat
- Fmea KarsDokumen54 halamanFmea Karsd_anto781063Belum ada peringkat
- Ehs PolicyDokumen27 halamanEhs Policylucky lukmanBelum ada peringkat
- Modul BR 2020 Risk Management Process2020Dokumen36 halamanModul BR 2020 Risk Management Process2020Maya AudinaBelum ada peringkat
- Fmea SigitDokumen36 halamanFmea Sigitantoapri28Belum ada peringkat
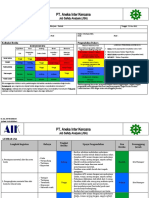
- JSA Gerinda PT - AIKDokumen4 halamanJSA Gerinda PT - AIKMhd Garry LuthfiBelum ada peringkat
- Fmea KarsDokumen54 halamanFmea KarsShinichi Kudo100% (2)
- Training FMEADokumen48 halamanTraining FMEAFajriRamadhanBelum ada peringkat
- LabKes - Bab 2 TKK (6-10)Dokumen22 halamanLabKes - Bab 2 TKK (6-10)Nanik AndianiBelum ada peringkat
- MR07 en IdDokumen12 halamanMR07 en IdMardianaBelum ada peringkat
- Analisa Risiko Dengan Metode FMEADokumen20 halamanAnalisa Risiko Dengan Metode FMEAfauzi ichvanBelum ada peringkat
- Penerapan Manajemen Risiko Terintegrasi Sesuai Standard Akreditasi 2024-KemkesDokumen21 halamanPenerapan Manajemen Risiko Terintegrasi Sesuai Standard Akreditasi 2024-KemkesAprilia ChrisBelum ada peringkat
- HFMEADokumen42 halamanHFMEAYanthee ParikasBelum ada peringkat
- HiraDokumen36 halamanHiraAri YusliandiBelum ada peringkat
- MKL2021 Kuliah#5Dokumen18 halamanMKL2021 Kuliah#5Ahmad RifqiBelum ada peringkat
- Bukti Fmea 2023Dokumen22 halamanBukti Fmea 2023pkmpucungBelum ada peringkat
- Fmea 2022Dokumen54 halamanFmea 2022Tatang KusnadiBelum ada peringkat
- P Sunarto Pertemuan Ke 2 Bidan (1) SalinanDokumen47 halamanP Sunarto Pertemuan Ke 2 Bidan (1) SalinanfaezalBelum ada peringkat
- HazopHazidDokumen54 halamanHazopHazidRyan SetiawanBelum ada peringkat
- Tools Manajemen Risiko - 1Dokumen60 halamanTools Manajemen Risiko - 1danauindahBelum ada peringkat
- Workshop FMEA External - 2021 - BatamDokumen96 halamanWorkshop FMEA External - 2021 - BatamQRM CikarangBelum ada peringkat
- Manajemen Mutu Di PuskesmasDokumen48 halamanManajemen Mutu Di PuskesmasM. Tito naruddin100% (6)
- Failure Mode - En.idDokumen144 halamanFailure Mode - En.idDosen AmaBelum ada peringkat
- Analisa Risiko Dengan Metode FMEADokumen20 halamanAnalisa Risiko Dengan Metode FMEAsandy hidayatBelum ada peringkat
- DR Hervita Fmea Kars - 244Dokumen54 halamanDR Hervita Fmea Kars - 244Piren SeptianmarBelum ada peringkat
- IBPR PIT EO1 Dumping Di Air MTN 031C IPC Mei 2018Dokumen22 halamanIBPR PIT EO1 Dumping Di Air MTN 031C IPC Mei 2018rifki bahtiarBelum ada peringkat
- Manajemen Mutu Di PuskesmasDokumen28 halamanManajemen Mutu Di PuskesmasVivin MulyatiBelum ada peringkat
- Manajemen Risiko Dalam Aspek Peningkatan Mutu Di KlinikDokumen20 halamanManajemen Risiko Dalam Aspek Peningkatan Mutu Di KlinikRudi HartantoBelum ada peringkat
- Manajemen Risiko Perbekalan Farmasi - PPT - CompressedDokumen68 halamanManajemen Risiko Perbekalan Farmasi - PPT - CompressednaradanagaBelum ada peringkat
- Risk Analysis MethodologiesDokumen75 halamanRisk Analysis MethodologiesRidzky Zul AsdiBelum ada peringkat
- Manajemen Mutu Di Puskesmas - GtoDokumen51 halamanManajemen Mutu Di Puskesmas - GtoFachrul Latif Dentist100% (2)
- Manajemen Resiko k3 Di RsDokumen33 halamanManajemen Resiko k3 Di RsDevina Arin KusumadewiBelum ada peringkat
- Analisa Risiko Dengan Metode FMEADokumen21 halamanAnalisa Risiko Dengan Metode FMEAAprilia ChrisBelum ada peringkat
- 13 - FmeaDokumen37 halaman13 - Fmeadenisa eoyBelum ada peringkat
- Materi FmeaDokumen28 halamanMateri FmeaMandalina SilalahiBelum ada peringkat
- Failure Mode and Effcet Analysis (Analisa Pro Aktif) : Dr. Luwiharsih, MSC Komisi Akreditasi Rumah SakitDokumen41 halamanFailure Mode and Effcet Analysis (Analisa Pro Aktif) : Dr. Luwiharsih, MSC Komisi Akreditasi Rumah Sakitevie manullangBelum ada peringkat
- Kisi-Kisi-pas PDO 2021 EdiDokumen13 halamanKisi-Kisi-pas PDO 2021 EdiBkk Jaya SentosaBelum ada peringkat
- MR - Severity Assessment FinalDokumen47 halamanMR - Severity Assessment Finallaboratorium pkm ambuntenBelum ada peringkat
- Indi MutuDokumen3 halamanIndi Mutukvmimila0Belum ada peringkat
- Infection Contro Risk Assesment (Icra)Dokumen31 halamanInfection Contro Risk Assesment (Icra)Nur IkhsanBelum ada peringkat
- Pendekatan Sistem PuskesmasDokumen13 halamanPendekatan Sistem PuskesmasaningBelum ada peringkat
- Manajemen Risiko Non KlinisDokumen46 halamanManajemen Risiko Non KlinisAhmad KoerniawanBelum ada peringkat
- Tra MethodDokumen27 halamanTra MethodFarid KurniadiBelum ada peringkat
- 9.1.1.8 Laporan Pelaksanaan Kegiatan FMEA Puskesmas Dumai KotaDokumen7 halaman9.1.1.8 Laporan Pelaksanaan Kegiatan FMEA Puskesmas Dumai KotaFlash YapBelum ada peringkat
- Praktek Penyusunan Kajian RisikoDokumen22 halamanPraktek Penyusunan Kajian Risikofebrian dwiBelum ada peringkat
- Analisis HFMEADokumen27 halamanAnalisis HFMEAnephylymBelum ada peringkat
- Materi 1 - Hilirisasi Produk Pemanfaatan Penginderaan JauhDokumen24 halamanMateri 1 - Hilirisasi Produk Pemanfaatan Penginderaan JauhSinta Ayu PuspaningrumBelum ada peringkat
- PERENCANAANDokumen15 halamanPERENCANAANajialimudine1Belum ada peringkat
- Modul K3 - Housekeeping, Manajemen Hiperkes Dan Keselamatan Kerja Di PerusahaanDokumen59 halamanModul K3 - Housekeeping, Manajemen Hiperkes Dan Keselamatan Kerja Di PerusahaanMuhammad SyamaniBelum ada peringkat
- Mutu Agreditasi PuskleDokumen25 halamanMutu Agreditasi PuskleBenosthian ErsandoBelum ada peringkat
- 1 Assmnt Mtce PusriDokumen55 halaman1 Assmnt Mtce PusrialexmontellBelum ada peringkat
- Manajemen Mutu Di PuskesmasDokumen48 halamanManajemen Mutu Di Puskesmasdiantriz095Belum ada peringkat
- Hiradc Terbaru KalimalangDokumen9 halamanHiradc Terbaru Kalimalangpriyo_arsen100% (1)
- TSI Bank 2 PDFDokumen31 halamanTSI Bank 2 PDFAdhis Darussalam PamungkasBelum ada peringkat
- Audit KasusDokumen26 halamanAudit KasusErwan SutrisnoBelum ada peringkat
- Perubahan Konsep Mutu Era JKNDokumen22 halamanPerubahan Konsep Mutu Era JKNFanniBelum ada peringkat
- FMEA RevDokumen116 halamanFMEA RevAldry Buvi Yvc-v'zeroFortysixBelum ada peringkat
- Registrasi Risiko RS: Hanevi Djasri, DR, Mars Eva Tirta Bayu Hasri, Skep, MPHDokumen17 halamanRegistrasi Risiko RS: Hanevi Djasri, DR, Mars Eva Tirta Bayu Hasri, Skep, MPHevie manullangBelum ada peringkat
- Failure Mode and Effect Analysis (Fmea) : Rsia Hermina Jatinegara 2013Dokumen31 halamanFailure Mode and Effect Analysis (Fmea) : Rsia Hermina Jatinegara 2013evie manullangBelum ada peringkat
- Pelanggaran Kode Etik Keperawatan RinganDokumen4 halamanPelanggaran Kode Etik Keperawatan Ringanevie manullangBelum ada peringkat
- Failure Mode and Effcet Analysis (Analisa Pro Aktif) : Dr. Luwiharsih, MSC Komisi Akreditasi Rumah SakitDokumen41 halamanFailure Mode and Effcet Analysis (Analisa Pro Aktif) : Dr. Luwiharsih, MSC Komisi Akreditasi Rumah Sakitevie manullangBelum ada peringkat
- Tim Pengendali MutuDokumen37 halamanTim Pengendali Mutuevie manullangBelum ada peringkat
- Bantex New LabelDokumen1 halamanBantex New Labelevie manullangBelum ada peringkat
- Surat Pengantar WS Keperawatan.Dokumen3 halamanSurat Pengantar WS Keperawatan.evie manullangBelum ada peringkat
- WS Keperawatan Gel 8 PalembangDokumen2 halamanWS Keperawatan Gel 8 Palembangevie manullangBelum ada peringkat
- WS KeperawatanDokumen1 halamanWS Keperawatanevie manullangBelum ada peringkat
- SE KARS No 408 TH 2020 Tentang Penundaan Kegiatan KARS Terkait Akreditasi PDFDokumen2 halamanSE KARS No 408 TH 2020 Tentang Penundaan Kegiatan KARS Terkait Akreditasi PDFevie manullangBelum ada peringkat
- RSUD Prambanan PDFDokumen7 halamanRSUD Prambanan PDFevie manullangBelum ada peringkat