Anda mungkin juga menyukai
- Tumor TelingaDokumen21 halamanTumor Telingahendra ardiantoBelum ada peringkat
- Neoplasia & Kanker KLDokumen31 halamanNeoplasia & Kanker KLshintaBelum ada peringkat
- Sss155 Slide Tumor TelingaDokumen23 halamanSss155 Slide Tumor TelingaWahyu IndartiBelum ada peringkat
- Lapsus Onko FixDokumen51 halamanLapsus Onko FixIgaMasPutriBelum ada peringkat
- Kelainan Pada RahangDokumen6 halamanKelainan Pada RahangAbi ZakiBelum ada peringkat
- Neoplasia & Kanker KL - PPSXDokumen139 halamanNeoplasia & Kanker KL - PPSXPaul IwawoBelum ada peringkat
- Keganasan Pada Kepala Leher Dan PenatalaksanaannyaDokumen46 halamanKeganasan Pada Kepala Leher Dan PenatalaksanaannyaNugraha WirawanBelum ada peringkat
- Tumor Hidung Dan Sinus Paranasal..AntiDokumen29 halamanTumor Hidung Dan Sinus Paranasal..AntiprincessismaBelum ada peringkat
- Kanker Kepala Dan LeherDokumen39 halamanKanker Kepala Dan LeherYASMINDPBelum ada peringkat
- Ca SinonasalDokumen28 halamanCa SinonasalMOH ABDUL FRENGKIBelum ada peringkat
- Materi 2 - Tumor Cavum Oris Dan Kelenjar LudahDokumen5 halamanMateri 2 - Tumor Cavum Oris Dan Kelenjar LudahFitrach AbdullahBelum ada peringkat
- NeoplasmaDokumen40 halamanNeoplasmalorensiafdBelum ada peringkat
- CA Sinonasal - Adlin Nadila FitalokaDokumen44 halamanCA Sinonasal - Adlin Nadila FitalokaAdlin NadilaBelum ada peringkat
- Tumor Meatus Akustikus ExternusDokumen28 halamanTumor Meatus Akustikus ExternusAkmal MukminBelum ada peringkat
- Responsi - Syadza Salsabila - 212011101041 - Tumor Kepala Dan LeherDokumen78 halamanResponsi - Syadza Salsabila - 212011101041 - Tumor Kepala Dan LeherLintang ApriliaBelum ada peringkat
- Onkologi THT - Modul 5.2 PDFDokumen43 halamanOnkologi THT - Modul 5.2 PDFPinguin SatuBelum ada peringkat
- Tumor ParotisDokumen51 halamanTumor Parotismelva paramitaBelum ada peringkat
- Bedah Kepala Dan LeherDokumen22 halamanBedah Kepala Dan LeherIndah Keyen'sBelum ada peringkat
- Referat Karsinoma TonsilDokumen21 halamanReferat Karsinoma TonsilSpica AdharaBelum ada peringkat
- Tumor SinonasalDokumen51 halamanTumor SinonasalKicky ChacaBelum ada peringkat
- CA NasofaringDokumen42 halamanCA NasofaringAfiyah putri zadaBelum ada peringkat
- Faktor Resiko & Deteksi Dini Kanker Mulut (Tichvy)Dokumen38 halamanFaktor Resiko & Deteksi Dini Kanker Mulut (Tichvy)Tichvy TammamaBelum ada peringkat
- BEDAH SLIDE Tumor ParotisDokumen31 halamanBEDAH SLIDE Tumor ParotisColineBelum ada peringkat
- Pembesaran Kelenjar Liur: Dr. Kamal Basri Siregar, SP.B (K) OnkDokumen56 halamanPembesaran Kelenjar Liur: Dr. Kamal Basri Siregar, SP.B (K) OnkAnonymous 1EQutBBelum ada peringkat
- Tumor Hidung Dan Sinus ParanasalDokumen20 halamanTumor Hidung Dan Sinus ParanasalWanda WardhaniBelum ada peringkat
- Keganasan Pada THTDokumen62 halamanKeganasan Pada THTRody KurniawanBelum ada peringkat
- Tumor Rongga MulutDokumen41 halamanTumor Rongga MulutWirdwtBelum ada peringkat
- Patofisiologi Neoplasma Sistem DigestifDokumen97 halamanPatofisiologi Neoplasma Sistem DigestifRaditya PrimaBelum ada peringkat
- IPM-8 Kanker MulutDokumen30 halamanIPM-8 Kanker MulutWilan Dita NesyiaBelum ada peringkat
- Neoplasma Jaringan Lunak MulutDokumen45 halamanNeoplasma Jaringan Lunak MulutHendry C R UlaenBelum ada peringkat
- Tumor Meatus Akustikus EksternusDokumen19 halamanTumor Meatus Akustikus EksternusAkmal MukminBelum ada peringkat
- Teori KNFDokumen26 halamanTeori KNFLaili Nur AzizahBelum ada peringkat
- IT 6 - Tumor Mata - IBDokumen64 halamanIT 6 - Tumor Mata - IBalviantiauliaBelum ada peringkat
- MODUL NEOPLASMA TELINGA + UNAS APRIL 2019 No. 41-50Dokumen45 halamanMODUL NEOPLASMA TELINGA + UNAS APRIL 2019 No. 41-50Daniel BramantyoBelum ada peringkat
- Referat Pleomorfik Adenoma ParotisDokumen23 halamanReferat Pleomorfik Adenoma ParotisCindy ClaudiaBelum ada peringkat
- Tumor ParotisDokumen29 halamanTumor ParotisFauziah LubisBelum ada peringkat
- Karsinoma TiroidDokumen19 halamanKarsinoma Tiroidratih agridithaBelum ada peringkat
- Onkologi Bedah Kepala Dan LeherDokumen108 halamanOnkologi Bedah Kepala Dan LeherAnonymous vxyyUu0MlZBelum ada peringkat
- Case Tumor Parotis MaskurDokumen50 halamanCase Tumor Parotis MaskurMasykur Ramadhan GaniBelum ada peringkat
- Tumor Hidung Dan Sinus ParanasalDokumen46 halamanTumor Hidung Dan Sinus Paranasalqiqifahria100% (1)
- Tumor RahangDokumen34 halamanTumor RahangAyu AnggayantiBelum ada peringkat
- Carcinoma Cavum Nasi RestuDokumen24 halamanCarcinoma Cavum Nasi Resturestupertiwi92Belum ada peringkat
- CA ParotisDokumen33 halamanCA ParotisHafizus SabriBelum ada peringkat
- Tumor SinonasalDokumen51 halamanTumor Sinonasalarini ABelum ada peringkat
- Tumor Lidah: Laporan KasusDokumen62 halamanTumor Lidah: Laporan KasusIgaMasPutriBelum ada peringkat
- Neoplasma Rongga MulutDokumen8 halamanNeoplasma Rongga MulutanjozzBelum ada peringkat
- PP Tumor Hidung & Sinus ParanasalDokumen22 halamanPP Tumor Hidung & Sinus ParanasalAnonymous REm9yuQABrBelum ada peringkat
- Kanker Kepala Dan Leher-1Dokumen33 halamanKanker Kepala Dan Leher-1yongkyBelum ada peringkat
- Tumor Regio ColliDokumen37 halamanTumor Regio ColliJeanna Salima100% (2)
- Tumor OtakDokumen62 halamanTumor OtakUunsariBelum ada peringkat
- Tumor ParotisDokumen41 halamanTumor ParotisRushda100% (1)
- Tumor GanasDokumen16 halamanTumor GanasBerlian KurniawatiBelum ada peringkat
- Lapsus Kanker LidahDokumen32 halamanLapsus Kanker LidahRido Jati KuncaraBelum ada peringkat
- Referat Parotis AlmustDokumen25 halamanReferat Parotis AlmustAli Sibra MulluziBelum ada peringkat
- Tumor SinonasalDokumen25 halamanTumor SinonasalcynthiaBelum ada peringkat
- BST - Pembesaran Kelenjar Air Liur (DR - Pimpin)Dokumen47 halamanBST - Pembesaran Kelenjar Air Liur (DR - Pimpin)Shusheelan KuppusamyBelum ada peringkat
- Bagan Penyakit Kulit XLVDokumen1 halamanBagan Penyakit Kulit XLVKelompok 5seBelum ada peringkat
- Buku Pneumonia COVID 19 - PDPI 2020 PDFDokumen67 halamanBuku Pneumonia COVID 19 - PDPI 2020 PDFamdita100% (3)
- Prevalensi Penyakit Tropik Infeksi 3 Tahun Terakhir Di Wilayah Jawa TimurDokumen1 halamanPrevalensi Penyakit Tropik Infeksi 3 Tahun Terakhir Di Wilayah Jawa TimurIcasiaYuseliBelum ada peringkat
- Sindroma Duh Tubuh Pria FIX PDFDokumen12 halamanSindroma Duh Tubuh Pria FIX PDFIcasiaYuseliBelum ada peringkat
- 1.1.Dr - Nasser-Ethical Issue in Daily Practice-Ilovepdf-CompressedDokumen25 halaman1.1.Dr - Nasser-Ethical Issue in Daily Practice-Ilovepdf-CompressedIcasiaYuseliBelum ada peringkat
- Penyuluhan Iva Dan SadanisDokumen26 halamanPenyuluhan Iva Dan SadanisIcasiaYuseliBelum ada peringkat
- 523 980 1 SM PDFDokumen6 halaman523 980 1 SM PDFWildan'z CreedBelum ada peringkat
- Definisi MenstruasiDokumen2 halamanDefinisi MenstruasiIcasiaYuseliBelum ada peringkat
- 523 980 1 SM PDFDokumen6 halaman523 980 1 SM PDFWildan'z CreedBelum ada peringkat
- Bab IDokumen7 halamanBab IfebrianaBelum ada peringkat
- FISIOLOGI MENSTRUASI Yang BenarDokumen1 halamanFISIOLOGI MENSTRUASI Yang BenarIcasiaYuseliBelum ada peringkat
- Anatomi Panggul Dan VTDokumen11 halamanAnatomi Panggul Dan VTIcasiaYuseliBelum ada peringkat
- Makro So MiaDokumen5 halamanMakro So MiarendyandromedaBelum ada peringkat
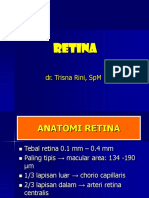
- Retina 2016Dokumen61 halamanRetina 2016ericawinataBelum ada peringkat
- Kuliah Tenggorok 1Dokumen54 halamanKuliah Tenggorok 1IcasiaYuseliBelum ada peringkat
- Hernia Inguinalis XXDokumen54 halamanHernia Inguinalis XXIcasiaYuseliBelum ada peringkat
- Retina 2016Dokumen61 halamanRetina 2016ericawinataBelum ada peringkat
- Filsafat HukumDokumen172 halamanFilsafat HukumIcasiaYuseli100% (1)
- Neuro OftalmologiDokumen71 halamanNeuro OftalmologiIcasiaYuseliBelum ada peringkat
- Soal Hiperkes Maret 2015Dokumen6 halamanSoal Hiperkes Maret 2015Nadya Yuniarti Dhp80% (5)
- Materi Kuliah External Eye DiseaseDokumen69 halamanMateri Kuliah External Eye DiseaseIcasiaYuseliBelum ada peringkat
- Perlindungan Hukum Bagi Penyelam Terhadap Keamanan Dan KeselamatanDokumen22 halamanPerlindungan Hukum Bagi Penyelam Terhadap Keamanan Dan KeselamatanIcasiaYuseliBelum ada peringkat
- Medika Legal Rekam MedisDokumen3 halamanMedika Legal Rekam MedisIcasiaYuseliBelum ada peringkat
- RefratDokumen2 halamanRefratIcasiaYuseliBelum ada peringkat
- Revisi Refrat Ica Editing 1Dokumen39 halamanRevisi Refrat Ica Editing 1IcasiaYuseliBelum ada peringkat
- MR 8-5-2016Dokumen59 halamanMR 8-5-2016IcasiaYuseliBelum ada peringkat
- Case Report Neuro SurgeryDokumen6 halamanCase Report Neuro SurgeryIcasiaYuseliBelum ada peringkat
- Morning Report 9 MaretDokumen16 halamanMorning Report 9 MaretIcasiaYuseliBelum ada peringkat
- Definisi MenstruasiDokumen2 halamanDefinisi MenstruasiIcasiaYuseliBelum ada peringkat