Anda mungkin juga menyukai
- CLEFT LIP PALATEDokumen39 halamanCLEFT LIP PALATEummiBelum ada peringkat
- Peritonitis GeneralisataDokumen21 halamanPeritonitis Generalisatawawan siswokoBelum ada peringkat
- Kel 3 PPT Penyuluhan Tentang Bibir SumbingDokumen15 halamanKel 3 PPT Penyuluhan Tentang Bibir SumbingAgita SpBelum ada peringkat
- CLP GenturDokumen96 halamanCLP Genturandika rafaelBelum ada peringkat
- CSS - Depressed FractureDokumen6 halamanCSS - Depressed FractureAyu Niken Savitri100% (1)
- Klasifikasi FlapDokumen29 halamanKlasifikasi FlapRocky NurakbariansyahBelum ada peringkat
- Referat Kelenjar LiurDokumen23 halamanReferat Kelenjar Liurahmad iffa maududyBelum ada peringkat
- T.O Colostomi AnakDokumen36 halamanT.O Colostomi AnakDionisius PwBelum ada peringkat
- Teknik Operasi HerniaDokumen2 halamanTeknik Operasi HerniaAndreas ChandraBelum ada peringkat
- Mar BSTDokumen8 halamanMar BSTFenny NurafniBelum ada peringkat
- Tinjauan PustakaDokumen5 halamanTinjauan PustakaMillatiazmi Maulida ArdianiBelum ada peringkat
- To MastektomiDokumen29 halamanTo Mastektomitepat rshsBelum ada peringkat
- LAPAROTOMYDokumen78 halamanLAPAROTOMYbamboomanBelum ada peringkat
- Fraktur PatellaDokumen24 halamanFraktur PatellaMeiria SariBelum ada peringkat
- ULKUS MARJOLINDokumen8 halamanULKUS MARJOLINTriantiMarthenParaBelum ada peringkat
- Fraktur Femur Pada AnakDokumen22 halamanFraktur Femur Pada AnakRexa Adie Sandy PoetraBelum ada peringkat
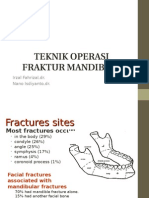
- TEKNIK OPERASI FRAKTUR MANDIBULADokumen19 halamanTEKNIK OPERASI FRAKTUR MANDIBULAicalBelum ada peringkat
- Teknik Operasi CraniotomiDokumen4 halamanTeknik Operasi CraniotomiAryo WibisonoBelum ada peringkat
- Kelainan KongenitalDokumen234 halamanKelainan KongenitalsmileyginaaBelum ada peringkat
- Tumor CaecumDokumen16 halamanTumor CaecumjihanBelum ada peringkat
- Tumor ParotisDokumen24 halamanTumor ParotisBanu WidagdoBelum ada peringkat
- TraumaToraksDokumen72 halamanTraumaToraksdilaBelum ada peringkat
- KSSKulitDokumen11 halamanKSSKulitSri WahyuniBelum ada peringkat
- Pedoman Bologna Untuk Diagnosis Dan Penatalaksanaan Adhesive Small Bowel ObstructionDokumen34 halamanPedoman Bologna Untuk Diagnosis Dan Penatalaksanaan Adhesive Small Bowel ObstructionAzwin KamarBelum ada peringkat
- LabiognatopalatoschizisDokumen38 halamanLabiognatopalatoschizisakbarsepadan100% (1)
- SPM Atresia JejunoilealDokumen2 halamanSPM Atresia JejunoilealIA Dwi Oka PutriBelum ada peringkat
- 3a. Prinsip-Prinsip Bedah OnkologiDokumen76 halaman3a. Prinsip-Prinsip Bedah OnkologiRizkia Alifa FitrianiBelum ada peringkat
- Trauma Abdomen Dan Pelvis, KuliahDokumen51 halamanTrauma Abdomen Dan Pelvis, KuliahAmmar Lukman MakarimBelum ada peringkat
- Terapi Modalitas Kanker PayudaraDokumen28 halamanTerapi Modalitas Kanker PayudaraAnonymous GCceOXiBelum ada peringkat
- Traksi ProstatDokumen35 halamanTraksi ProstatHezar SalahudinBelum ada peringkat
- Akse Bedah Pada Bedah DigestifDokumen78 halamanAkse Bedah Pada Bedah DigestifRyan Luqman H100% (1)
- Clipp Cot FinDokumen14 halamanClipp Cot Finagung mapBelum ada peringkat
- 9 - Prinsip Tindakan Bedah OnkologiDokumen13 halaman9 - Prinsip Tindakan Bedah OnkologiSitiFitiahBelum ada peringkat
- Tumor IDEM - En.idDokumen8 halamanTumor IDEM - En.idDarmawan Eko FerryBelum ada peringkat
- Tumor Patudara BKDokumen46 halamanTumor Patudara BKSuryadi VOoBelum ada peringkat
- HIPOSPADIADokumen55 halamanHIPOSPADIABedahanakugmBelum ada peringkat
- Amputasi DM Komplikasi dan PencegahanDokumen10 halamanAmputasi DM Komplikasi dan PencegahanShilny MBelum ada peringkat
- Tiroid SurabayaDokumen57 halamanTiroid SurabayavalentinoBelum ada peringkat
- Reduksi TerbukaDokumen3 halamanReduksi TerbukaTimmy Sie Muslimah SedjatieBelum ada peringkat
- Fraktur Basis CraniiDokumen2 halamanFraktur Basis CraniiAlvin JiwonoBelum ada peringkat
- Fraktur MaksilofasialDokumen29 halamanFraktur MaksilofasialIndah NababanBelum ada peringkat
- Anatomi FaceiDokumen48 halamanAnatomi FaceiAnonymous v2aJxfe9RzBelum ada peringkat
- KONTRAKTUR DIGITIDokumen36 halamanKONTRAKTUR DIGITITsamara YumnaBelum ada peringkat
- Abses PeritonsilDokumen27 halamanAbses Peritonsilnot_a_geekBelum ada peringkat
- Fraktur Impresi:depresiDokumen5 halamanFraktur Impresi:depresiSurahman Hadi100% (1)
- Fraktur Head RadiusDokumen36 halamanFraktur Head RadiusRajaAnjuPratamaPardedeBelum ada peringkat
- Kuliah Bedah Plastik IDokumen41 halamanKuliah Bedah Plastik IIntan Hanifah MutmainnahBelum ada peringkat
- Palatoplasti Dengan Metode Push BackDokumen25 halamanPalatoplasti Dengan Metode Push BackMaulanaAdjieIbrahimBelum ada peringkat
- Edit Teknik Operasi Batu Ginjal YESDokumen41 halamanEdit Teknik Operasi Batu Ginjal YESIrfanHadiWijayaBelum ada peringkat
- Materi KuliahDokumen92 halamanMateri KuliahMaharani100% (1)
- FRKTUR DEPRESI DAN KONTUSI SEREBRIDokumen28 halamanFRKTUR DEPRESI DAN KONTUSI SEREBRIKurnia Sari0% (1)
- Hernia Inguinalis Lateralis Dextra IreponibleDokumen13 halamanHernia Inguinalis Lateralis Dextra Ireponiblegaluh ajeng firstyBelum ada peringkat
- AMPUTASI EKSTREMITAS BAWAHDokumen52 halamanAMPUTASI EKSTREMITAS BAWAHMuhammad RezaBelum ada peringkat
- BIBIR SUMBINGDokumen20 halamanBIBIR SUMBINGKiki FernandoBelum ada peringkat
- Intususepsi Dan ManajemenDokumen11 halamanIntususepsi Dan ManajemenAyu PermataBelum ada peringkat
- Cara Mengatasi Masalah Pada Cleft Lip Dan PalateDokumen73 halamanCara Mengatasi Masalah Pada Cleft Lip Dan PalateNor AinaBelum ada peringkat
- Kuliah CLP 2016Dokumen49 halamanKuliah CLP 2016Adena Riskivia TrinandaBelum ada peringkat
- Cara Mengatasi LabiopalatognatoschisisDokumen30 halamanCara Mengatasi Labiopalatognatoschisishannya manBelum ada peringkat
- Tanya CLPDokumen17 halamanTanya CLPSukuria UsmanBelum ada peringkat
- Cara Mengatasi Cleft Lip dan PalateDokumen37 halamanCara Mengatasi Cleft Lip dan PalatealterBelum ada peringkat
- BAB 1. PendahuluanDokumen2 halamanBAB 1. PendahuluangratianusbBelum ada peringkat
- Cover Fix Mini ProDokumen8 halamanCover Fix Mini ProgratianusbBelum ada peringkat
- BAB 3. Metodologi PenelitianDokumen3 halamanBAB 3. Metodologi PenelitiangratianusbBelum ada peringkat
- PDFDokumen61 halamanPDFAs RifahBelum ada peringkat
- BAB 4. Hasil Dan PembahsanDokumen3 halamanBAB 4. Hasil Dan PembahsangratianusbBelum ada peringkat
- Penelitian UGM TB AnakDokumen6 halamanPenelitian UGM TB AnakRaymond Efraim NgkaleBelum ada peringkat
- BAB 1. PendahuluanDokumen2 halamanBAB 1. PendahuluangratianusbBelum ada peringkat
- BAB 2. Tinjauan PustakaDokumen12 halamanBAB 2. Tinjauan PustakagratianusbBelum ada peringkat
- Pengobatan Terkini Sindrom Nefrotik Pada AnakDokumen8 halamanPengobatan Terkini Sindrom Nefrotik Pada AnakToto HandayonoBelum ada peringkat
- Kerangka TeoriDokumen2 halamanKerangka TeorigratianusbBelum ada peringkat
- PDFDokumen61 halamanPDFAs RifahBelum ada peringkat
- Manajemen Puskesmas 2013Dokumen49 halamanManajemen Puskesmas 2013gratianusbBelum ada peringkat
- SN Bab IiDokumen28 halamanSN Bab IigratianusbBelum ada peringkat
- BAB 5. Simpulan Dan SaranDokumen1 halamanBAB 5. Simpulan Dan SarangratianusbBelum ada peringkat
- Penyakit Tuberkulosis Paru Dan SistemikDokumen55 halamanPenyakit Tuberkulosis Paru Dan SistemikErvina Lie100% (1)
- SATELIT SIMPOSIUM 6.1 DM UPDATE DAN Hb1C OLEH DR. Dr. Fatimah Eliana SPPD KEMD PDFDokumen7 halamanSATELIT SIMPOSIUM 6.1 DM UPDATE DAN Hb1C OLEH DR. Dr. Fatimah Eliana SPPD KEMD PDFHipoAflisBelum ada peringkat
- PMK No. 15 TTG Penanggulangan CacinganDokumen78 halamanPMK No. 15 TTG Penanggulangan CacinganpalangBelum ada peringkat
- Mental RetardasiDokumen35 halamanMental RetardasiThieFeezaeBelum ada peringkat
- Bab IiDokumen4 halamanBab IigratianusbBelum ada peringkat
- Bab IiiDokumen1 halamanBab IiigratianusbBelum ada peringkat
- Sken 4 Tut 1Dokumen2 halamanSken 4 Tut 1gratianusbBelum ada peringkat
- IKA Neonatal SepsisDokumen43 halamanIKA Neonatal SepsisgratianusbBelum ada peringkat
- Bab IDokumen2 halamanBab IgratianusbBelum ada peringkat
- Daftar IsiDokumen1 halamanDaftar IsigratianusbBelum ada peringkat
- Infanticid by Dr. IwanDokumen28 halamanInfanticid by Dr. IwangratianusbBelum ada peringkat
- IkterusDokumen3 halamanIkterusAlmira Shabrina SaraswatiBelum ada peringkat
- Sken 3 Tut 1Dokumen3 halamanSken 3 Tut 1gratianusbBelum ada peringkat
- Sken 1 Tut 1Dokumen2 halamanSken 1 Tut 1gratianusbBelum ada peringkat
- Tugas IKA Kel 1 - ApgarDokumen2 halamanTugas IKA Kel 1 - ApgarAlmira Shabrina SaraswatiBelum ada peringkat
- Sken 2 Tut 1&2Dokumen12 halamanSken 2 Tut 1&2gratianusbBelum ada peringkat