Anda mungkin juga menyukai
- HematologyDokumen36 halamanHematologyEmil LasulikaBelum ada peringkat
- HemostasisDokumen64 halamanHemostasisClarasintya ClarasintyaBelum ada peringkat
- TrombositDokumen23 halamanTrombositOh SehunnnBelum ada peringkat
- Trombosit 2024Dokumen26 halamanTrombosit 2024Fahmi AhmadBelum ada peringkat
- Erythrocyte and DiseaseDokumen122 halamanErythrocyte and DiseaseAhmad AnshoriBelum ada peringkat
- Studi Kasus HematologiDokumen24 halamanStudi Kasus HematologiWinda MuliawatiBelum ada peringkat
- 4 TrombositDokumen17 halaman4 TrombositMilla Artika IIBelum ada peringkat
- HematologiDokumen62 halamanHematologiStephaniePanyBelum ada peringkat
- K16 - Polisitemia Vera (Trombositosis & Eritrositosis)Dokumen39 halamanK16 - Polisitemia Vera (Trombositosis & Eritrositosis)Livia HanisamurtiBelum ada peringkat
- Kelainan TrombositDokumen23 halamanKelainan TrombositNurul HafizahBelum ada peringkat
- KP 2.1.4.3 - Diatesis Hemoragik (DIC, Trombositopenia, ITP, Hemofilia, Von Willebrand Diseases)Dokumen39 halamanKP 2.1.4.3 - Diatesis Hemoragik (DIC, Trombositopenia, ITP, Hemofilia, Von Willebrand Diseases)fitri juliantiBelum ada peringkat
- Trombosit FK UKIDokumen76 halamanTrombosit FK UKIVira HeumasseBelum ada peringkat
- Pemicu 2 Ferrel HematologiDokumen161 halamanPemicu 2 Ferrel HematologiFerrel Brilliyant UrsulaBelum ada peringkat
- Patofisiologi Hematologi 2017Dokumen44 halamanPatofisiologi Hematologi 2017nawrah afriBelum ada peringkat
- Kelainan TrombositDokumen23 halamanKelainan TrombositpuputBelum ada peringkat
- Sistem DarahDokumen37 halamanSistem Darah099 Devana Inaja ArifinBelum ada peringkat
- Sel ImatureDokumen50 halamanSel ImatureAngelia Rambu HamuBelum ada peringkat
- 3 - Kelainan HemostasisDokumen55 halaman3 - Kelainan HemostasisMandaBelum ada peringkat
- TROMBOSITOSISDokumen26 halamanTROMBOSITOSISChandra hidayatBelum ada peringkat
- Rangkuman Kelainan TrombositDokumen5 halamanRangkuman Kelainan TrombositginaBelum ada peringkat
- BAPER 2.3 Skenario 1Dokumen6 halamanBAPER 2.3 Skenario 1MOCH AR-ROSYID AZMIE PUTRA -Belum ada peringkat
- HemopoesisDokumen54 halamanHemopoesisXenaBelum ada peringkat
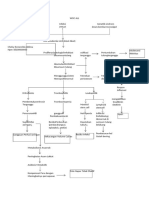
- Woc Leukemia 2Dokumen2 halamanWoc Leukemia 2Fujie HastutiBelum ada peringkat
- Pemeriksaan HemostasisDokumen78 halamanPemeriksaan HemostasisLaboratorium RSMP IndramayuBelum ada peringkat
- 2-Sistem DarahDokumen37 halaman2-Sistem DarahBunga Adhelia MaharaniBelum ada peringkat
- Pembentukan Trombus - Yoke - PresentasiDokumen46 halamanPembentukan Trombus - Yoke - PresentasiAkeBelum ada peringkat
- HematopoiesisDokumen35 halamanHematopoiesisMutia Fitri HafilizaraBelum ada peringkat
- 4 TrombositDokumen8 halaman4 Trombositolivia mardhani putriBelum ada peringkat
- Fisiologi TrombositDokumen7 halamanFisiologi TrombositIra Dwi NovriyantiBelum ada peringkat
- Sistem DarahDokumen37 halamanSistem DarahadityaBelum ada peringkat
- Hematopoesis - Dr. SuryantoDokumen5 halamanHematopoesis - Dr. SuryantoJamaluddin Ahmad A.M100% (1)
- GGN Hemostasis (Kuliah 5)Dokumen44 halamanGGN Hemostasis (Kuliah 5)Muhammad DelfinBelum ada peringkat
- PP Haematopoesis SusiDokumen60 halamanPP Haematopoesis Susiclaudya zaraBelum ada peringkat
- Referat ItpDokumen26 halamanReferat ItpNovianaHartikasariBelum ada peringkat
- LP Itp DeviDokumen24 halamanLP Itp DeviDevi SitudewiBelum ada peringkat
- Kuliah Kelainan Fungsi Trombosit - DyhDokumen45 halamanKuliah Kelainan Fungsi Trombosit - DyhdessyBelum ada peringkat
- Dr. IDA TrombositDokumen62 halamanDr. IDA TrombositSila DarmanaBelum ada peringkat
- 4.morfologi TrombositDokumen16 halaman4.morfologi TrombositHasmiddar100% (1)
- Patway 2Dokumen3 halamanPatway 2shafrina10032005Belum ada peringkat
- Patofisiologi Hematologi 2017Dokumen44 halamanPatofisiologi Hematologi 2017radiani100% (1)
- LP Itp Devi SintiaDokumen18 halamanLP Itp Devi SintiaDevi SitudewiBelum ada peringkat
- Kelompok 18 - Kelainan Sel TrombositDokumen19 halamanKelompok 18 - Kelainan Sel TrombositNima AufaBelum ada peringkat
- Pemicu 4 Blok HematologiDokumen94 halamanPemicu 4 Blok HematologiJessica Buntara SulaimanBelum ada peringkat
- Referat TrombositopeniaDokumen23 halamanReferat TrombositopeniaDhia UlfajriBelum ada peringkat
- TROMBOSITOPENIADokumen77 halamanTROMBOSITOPENIASiti AlfianaBelum ada peringkat
- Askep HematologiDokumen45 halamanAskep HematologiTriani HeriyantyBelum ada peringkat
- Leukemia & ThalassemiaDokumen31 halamanLeukemia & ThalassemiaMetha KemalaBelum ada peringkat
- Hemostasis UnmalDokumen61 halamanHemostasis UnmalIntan RizkaBelum ada peringkat
- Patofisiologi Sist. Hematologi AnakDokumen30 halamanPatofisiologi Sist. Hematologi AnakSTIKES BORNEO CENDEKIA MEDIKABelum ada peringkat
- Gangguan HemodinamikDokumen100 halamanGangguan HemodinamikAndi IrgiBelum ada peringkat
- Laporan Kasus Anak A Dengan Acute Myeloid LeukimiaDokumen31 halamanLaporan Kasus Anak A Dengan Acute Myeloid LeukimiaDevi Puri SukmawatiBelum ada peringkat
- Hematopoeisis Dan Morfologi DarahDokumen78 halamanHematopoeisis Dan Morfologi DarahJinani FirdausiyahBelum ada peringkat
- HematologiDokumen106 halamanHematologiAlicia AngelinaBelum ada peringkat
- 4 PK Leukemia DR Diah Revisi2Dokumen65 halaman4 PK Leukemia DR Diah Revisi2Nindya Agustin RBelum ada peringkat
- Ranitidine Terhadap TrombositopeniaDokumen19 halamanRanitidine Terhadap TrombositopeniaMimba WibiyanaBelum ada peringkat
- Gangguan Pada EritrositDokumen37 halamanGangguan Pada EritrositResta MahesaBelum ada peringkat
- Morfologi SelDokumen27 halamanMorfologi Selmirza juandaBelum ada peringkat
- Doctor SafetyDokumen16 halamanDoctor SafetyFadilah FadilahBelum ada peringkat
- Tugas Kuliah-Makalah SKN-Fadilah Nurulhuda H1A019036Dokumen11 halamanTugas Kuliah-Makalah SKN-Fadilah Nurulhuda H1A019036Fadilah FadilahBelum ada peringkat
- Kuesionare BaekceDokumen11 halamanKuesionare BaekceFadilah FadilahBelum ada peringkat
- Salinan Terjemahan Baecke - Questionnaire - For - Measurement - of - A - Person's - Habitual - Physical - ActivityDokumen6 halamanSalinan Terjemahan Baecke - Questionnaire - For - Measurement - of - A - Person's - Habitual - Physical - ActivityFadilah Fadilah100% (1)
- 416-Article Text-993-1-10-20220131Dokumen8 halaman416-Article Text-993-1-10-20220131Fadilah FadilahBelum ada peringkat
- 1139 4511 1 PBDokumen11 halaman1139 4511 1 PBFadilah FadilahBelum ada peringkat
- RAMA 11201 04011381823207 0017098502 0227108501 01 Front RefDokumen36 halamanRAMA 11201 04011381823207 0017098502 0227108501 01 Front RefFadilah FadilahBelum ada peringkat
- Juknis Persiapan Ke PuskesmasDokumen38 halamanJuknis Persiapan Ke PuskesmasFadilah FadilahBelum ada peringkat
- Pengumuman 1655172589 FileDokumen49 halamanPengumuman 1655172589 FileFadilah FadilahBelum ada peringkat
- 4604-Article Text-27760-1-10-20220629Dokumen8 halaman4604-Article Text-27760-1-10-20220629Fadilah FadilahBelum ada peringkat
- Essay IsmkiDokumen2 halamanEssay IsmkiFadilah FadilahBelum ada peringkat
- e75cfdb6-e50a-4d19-84e4-8f80c7124548Dokumen18 halamane75cfdb6-e50a-4d19-84e4-8f80c7124548Fadilah FadilahBelum ada peringkat
- Matriks Kelas BDokumen1 halamanMatriks Kelas BFadilah FadilahBelum ada peringkat