Anda mungkin juga menyukai
- Morning Report TBCDokumen12 halamanMorning Report TBCPingKikiBelum ada peringkat
- Pendekatan Diagnosis IkterusDokumen30 halamanPendekatan Diagnosis IkterusEvy LiesniawatiBelum ada peringkat
- Laporan Kasus HipertiroidDokumen50 halamanLaporan Kasus HipertiroidEkaBelum ada peringkat
- Lapkas Kolelitiasis Dr. MarintanDokumen36 halamanLapkas Kolelitiasis Dr. MarintanTia monikaBelum ada peringkat
- FINAL - Guideline COVID PERKI 9 Mei 2020 - REV PDFDokumen110 halamanFINAL - Guideline COVID PERKI 9 Mei 2020 - REV PDFbella labibahBelum ada peringkat
- Laporan Kasus GeriatriDokumen40 halamanLaporan Kasus GeriatriFahmi IbrahimBelum ada peringkat
- Displipid NewDokumen27 halamanDisplipid New최연기Belum ada peringkat
- Gangguan MakanDokumen14 halamanGangguan MakanKomang JananuragaBelum ada peringkat
- Case Report Demam TifoidDokumen21 halamanCase Report Demam TifoidHusni Andi100% (1)
- Referat DHFDokumen28 halamanReferat DHFAjeng Tri Septiani100% (1)
- Penyuluhan ProlanisDokumen33 halamanPenyuluhan ProlanisambarBelum ada peringkat
- Manifestasi Kulit Pada Pasien HIVDokumen7 halamanManifestasi Kulit Pada Pasien HIVBramantra TangsakhaBelum ada peringkat
- Laporan Kasus Kecil - Chorea AtetosisDokumen11 halamanLaporan Kasus Kecil - Chorea AtetosisKatarina Dewi SartikaBelum ada peringkat
- Referat Manajemen HipertensiDokumen15 halamanReferat Manajemen Hipertensisalsabila mustikaBelum ada peringkat
- Laporan Kasus KeratitisDokumen53 halamanLaporan Kasus KeratitisMaria EnjelinaBelum ada peringkat
- LAPSUS General AnestesiDokumen6 halamanLAPSUS General AnestesiadiningtitisBelum ada peringkat
- Sari Kepustakaan PAIDokumen15 halamanSari Kepustakaan PAIx22xBelum ada peringkat
- Referat Leptospirosis - JuliaDokumen36 halamanReferat Leptospirosis - JuliajuliaBelum ada peringkat
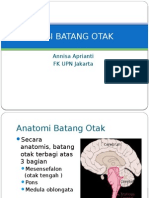
- Lesi Batang OtakDokumen21 halamanLesi Batang OtakAnnisa ApriantiBelum ada peringkat
- Diabetes Melitus Dan Gagal JantungDokumen20 halamanDiabetes Melitus Dan Gagal JantungsarahBelum ada peringkat
- Pitiriasis VersikolorDokumen24 halamanPitiriasis VersikolorRanty Femilya UtamiBelum ada peringkat
- PANSSDokumen4 halamanPANSSDevina Aulia AzizaBelum ada peringkat
- Tatalaksana Diagnosis Praktis AnemiaDokumen15 halamanTatalaksana Diagnosis Praktis AnemiaAnastasyaLianBelum ada peringkat
- Referat Mata Merah Visus Normal TaniaDokumen43 halamanReferat Mata Merah Visus Normal TaniaAngelina Tania Woda LadoBelum ada peringkat
- Status Ujian Obgyn RifkaDokumen13 halamanStatus Ujian Obgyn RifkarifkaraihanaBelum ada peringkat
- Puskesmas Waiwadan PedomanDokumen22 halamanPuskesmas Waiwadan PedomanEpank RosikiBelum ada peringkat
- Responsi GnapsDokumen16 halamanResponsi GnapsAnas JatikusumaBelum ada peringkat
- BST Irfan - CHF - CPC - Trombostosis Essensial - BPHDokumen67 halamanBST Irfan - CHF - CPC - Trombostosis Essensial - BPHGhaidaBelum ada peringkat
- Referat Congestive Heart Failure Pada Geriatri: Pembimbing Dr. Budi Enoch, Sp. PDDokumen20 halamanReferat Congestive Heart Failure Pada Geriatri: Pembimbing Dr. Budi Enoch, Sp. PDAriyanaBelum ada peringkat
- Laporan Kasus Psoriasis VulgarisDokumen24 halamanLaporan Kasus Psoriasis VulgarismarcoBelum ada peringkat
- GNAPSDokumen59 halamanGNAPSferinanatasyaBelum ada peringkat
- ADHDDokumen32 halamanADHDAYu MiFtakhunBelum ada peringkat
- Laporan Kasus GMP Akibat Zat MultipleDokumen15 halamanLaporan Kasus GMP Akibat Zat MultipleMunifa Magfhira NurseriBelum ada peringkat
- Efusi Pleura MasifDokumen25 halamanEfusi Pleura MasifAdeTriansyahEmsilBelum ada peringkat
- Referat HTDokumen18 halamanReferat HTDwi Aprila PutriBelum ada peringkat
- (Mini Project) SMP Sunan Giri - Puskesmas Cebongan - NapzaDokumen25 halaman(Mini Project) SMP Sunan Giri - Puskesmas Cebongan - Napzaal furqonBelum ada peringkat
- Pemeriksaan Dan Tata Laksana InsulinomaDokumen6 halamanPemeriksaan Dan Tata Laksana InsulinomaPutri HardyantiBelum ada peringkat
- Referat Ipd Hema MelenaDokumen10 halamanReferat Ipd Hema MelenaaullllllBelum ada peringkat
- KKD Rumple LeadDokumen28 halamanKKD Rumple LeadRaisya alandaBelum ada peringkat
- Referat HivDokumen44 halamanReferat HivMentari Dwi PutriBelum ada peringkat
- Case Status AsmatikusDokumen43 halamanCase Status AsmatikusWulan Sari CahyaniBelum ada peringkat
- Hemoroid CaseDokumen35 halamanHemoroid CaseMei SyaharaBelum ada peringkat
- Usg HeparDokumen20 halamanUsg HeparjoandreBelum ada peringkat
- Crs TonsilitisDokumen23 halamanCrs TonsilitisRahmidatul AftikaBelum ada peringkat
- Status Pasien Ujian OsteoarthritisDokumen9 halamanStatus Pasien Ujian OsteoarthritisCindy AmaliaBelum ada peringkat
- Presentasi Referat HipoglikemiaDokumen28 halamanPresentasi Referat Hipoglikemiaesti_mahananiBelum ada peringkat
- Penyakit Degeneratif FixDokumen26 halamanPenyakit Degeneratif FixrzkrfndniBelum ada peringkat
- Slide Stroke Hemoragik KitaDokumen77 halamanSlide Stroke Hemoragik KitaChaca NatashaBelum ada peringkat
- Family FolderDokumen33 halamanFamily FolderGalih Ayu PratiwiBelum ada peringkat
- Case Report SkizofreniaDokumen13 halamanCase Report SkizofreniaAyesha SiahaanBelum ada peringkat
- HepatomaDokumen30 halamanHepatomaAnonymous GTcrX5dRHBelum ada peringkat
- Refrat Syok Pada AnakDokumen75 halamanRefrat Syok Pada AnakV15CERA FK UNANDBelum ada peringkat
- Laporan Kasus Henoch Schonlein Purpura (HSP) Oleh Ahimsa Yoga AninditaDokumen25 halamanLaporan Kasus Henoch Schonlein Purpura (HSP) Oleh Ahimsa Yoga AninditaAhimsa Yoga AninditaBelum ada peringkat
- 13 Fos22 Patologi PersalinanDokumen60 halaman13 Fos22 Patologi Persalinanshare fos100% (1)
- Endokarditis InfektifDokumen45 halamanEndokarditis InfektifMuhammad Firdaus J KarimiBelum ada peringkat
- Hepatitis Viral AkutDokumen21 halamanHepatitis Viral AkutalitharachmaBelum ada peringkat
- Laporan Kasus HemoroidDokumen8 halamanLaporan Kasus HemoroidRizky Huryamin100% (1)
- Prof. Syarifuddin Sindrom Nefrotik Pada Anak (Kelas A)Dokumen43 halamanProf. Syarifuddin Sindrom Nefrotik Pada Anak (Kelas A)Michael HusainBelum ada peringkat
- Sindrom Nefrotik Pada AnakDokumen72 halamanSindrom Nefrotik Pada AnakZulkifli RahmanBelum ada peringkat
- Sari Pustaka - Anemia Pada CKD - Lavenia Zabrina - 2365050081Dokumen41 halamanSari Pustaka - Anemia Pada CKD - Lavenia Zabrina - 2365050081Dheby PasoroBelum ada peringkat
- Trombosis Vena Dalam Dan Emboli ParuDokumen24 halamanTrombosis Vena Dalam Dan Emboli ParuilvaBelum ada peringkat
- Trombosis Vena Dalam Dan Emboli ParuDokumen24 halamanTrombosis Vena Dalam Dan Emboli ParuilvaBelum ada peringkat
- Trombosis Vena Dalam Dan Emboli ParuDokumen24 halamanTrombosis Vena Dalam Dan Emboli ParuilvaBelum ada peringkat
- Pengertian Dan Klasifikasi KeputihanDokumen2 halamanPengertian Dan Klasifikasi KeputihanilvaBelum ada peringkat
- Chronic Kidney Disease PPT (Ilva, 07)Dokumen18 halamanChronic Kidney Disease PPT (Ilva, 07)ilvaBelum ada peringkat
- ISK (DR - Prema)Dokumen31 halamanISK (DR - Prema)rumaisyah alkatiriBelum ada peringkat
- Dr. Nanang - Pemeriksaan Pemeriksaan Autoimmune Masa Kini Dan Masa Yang Akan Datang Rev PDFDokumen65 halamanDr. Nanang - Pemeriksaan Pemeriksaan Autoimmune Masa Kini Dan Masa Yang Akan Datang Rev PDFNururrohmahBelum ada peringkat
- Bias Dalam Penelitian PKG PrintDokumen45 halamanBias Dalam Penelitian PKG PrintRisa SasmitaBelum ada peringkat
- CRS Preoperative AssessmentDokumen12 halamanCRS Preoperative AssessmentAnnisa WidjanarkoBelum ada peringkat
- Tugas Koas Gilut - Eddy YuristoDokumen15 halamanTugas Koas Gilut - Eddy YuristoDky HartonoBelum ada peringkat