Anda mungkin juga menyukai
- LITREV JantungDokumen13 halamanLITREV Jantungfrima rizky adyatmaBelum ada peringkat
- Resume Jurnal Bahasa InggrisDokumen3 halamanResume Jurnal Bahasa InggrisSyahrani AvrilBelum ada peringkat
- Journal Reading BEDAH FixDokumen13 halamanJournal Reading BEDAH FixrandaifaBelum ada peringkat
- Jurnal Interna Severe Covid-19Dokumen17 halamanJurnal Interna Severe Covid-19Alen TutuparyBelum ada peringkat
- Jurnal I Putu GunungDokumen15 halamanJurnal I Putu GunungPutu GunoengBelum ada peringkat
- Tugas Mangement ICU Destania - 20201030033Dokumen8 halamanTugas Mangement ICU Destania - 20201030033destania wardaniBelum ada peringkat
- Tugas Uts Managemen Yankes Novia Sri DamayantiDokumen6 halamanTugas Uts Managemen Yankes Novia Sri DamayantiNovia sridamayantiBelum ada peringkat
- Journal Reading AnestesiDokumen8 halamanJournal Reading Anestesimuhammad jihad biladuddinBelum ada peringkat
- Kegawatdaruratan Kardiovaskular Pada Covid 19Dokumen45 halamanKegawatdaruratan Kardiovaskular Pada Covid 19Rezza TikaBelum ada peringkat
- Jurnal DeliriumDokumen8 halamanJurnal DeliriumSabrina brinBelum ada peringkat
- Main en IdDokumen11 halamanMain en Idmuhammad yusuf deny faisalBelum ada peringkat
- COVID-19 MaretDokumen30 halamanCOVID-19 MaretAmran suparmanBelum ada peringkat
- Panduan - 1. Panduan Mutu - 3. Panduan PPI - 2. PANDUAN COVID 19Dokumen17 halamanPanduan - 1. Panduan Mutu - 3. Panduan PPI - 2. PANDUAN COVID 19Izda WatiBelum ada peringkat
- en IdDokumen11 halamanen Idmuhammad yusuf deny faisalBelum ada peringkat
- Jurnal Reading SarafDokumen21 halamanJurnal Reading SarafchewanBelum ada peringkat
- Vaksin Covid Ibu HamilDokumen10 halamanVaksin Covid Ibu HamilTitin PrihartiniBelum ada peringkat
- LP N4Dokumen22 halamanLP N4rezzaBelum ada peringkat
- ASkep CovidDokumen39 halamanASkep CoviddedyBelum ada peringkat
- Proposal Penelitian Dosen PemulaDokumen28 halamanProposal Penelitian Dosen PemulaAri KurniawanBelum ada peringkat
- 041 - Firman Satya P - Kep - GadarDokumen15 halaman041 - Firman Satya P - Kep - GadarFIRMAN SATYA PRADIPTABelum ada peringkat
- RS X SPO Pelayanan Pada Pasien Covid RevisiDokumen6 halamanRS X SPO Pelayanan Pada Pasien Covid RevisiekaBelum ada peringkat
- Referat - Tromboemboli Pada Covid 19Dokumen18 halamanReferat - Tromboemboli Pada Covid 19Widya MahiBelum ada peringkat
- Jurnal Stroke Ischemic Acute With COVID-19-Elizabeth TeteleptaDokumen39 halamanJurnal Stroke Ischemic Acute With COVID-19-Elizabeth TeteleptaDunia MedisBelum ada peringkat
- Managemen Fasilitas KesehatanDokumen6 halamanManagemen Fasilitas KesehatanRini Eka PutriBelum ada peringkat
- Jurding AnesDokumen7 halamanJurding AnesVania Revanita ManullangBelum ada peringkat
- Juring BM Vanti Rev2Dokumen38 halamanJuring BM Vanti Rev2Rivanti TariganBelum ada peringkat
- Asuhan Keperawatan Kritis Pasien Covid-19 AprilDokumen42 halamanAsuhan Keperawatan Kritis Pasien Covid-19 AprilNeneng ilah rohilahBelum ada peringkat
- Referat RJP Di Masa PandemiDokumen27 halamanReferat RJP Di Masa PandemilindaBelum ada peringkat
- Early Warning System Covid-19Dokumen43 halamanEarly Warning System Covid-19Dhian PramanaBelum ada peringkat
- Pedoman Pencegahan, Pengendalian Dan Tatalaksana Covid-19 Di Poltekbang SbyDokumen29 halamanPedoman Pencegahan, Pengendalian Dan Tatalaksana Covid-19 Di Poltekbang SbyKLINIK POLTEKBANGBelum ada peringkat
- Pengaruh Coronavirus Disease 2019 (COVID-19) Terhadap Insidens Dan Tatalaksana Penyakit SerebrovaskularDokumen6 halamanPengaruh Coronavirus Disease 2019 (COVID-19) Terhadap Insidens Dan Tatalaksana Penyakit SerebrovaskularIn-House Clinic PTMIBelum ada peringkat
- Tugas Journal Reading Rehabilitasi MedikDokumen6 halamanTugas Journal Reading Rehabilitasi MedikHerlina Kusuma DewiBelum ada peringkat
- Laporan Akhir Tugas SiapDokumen25 halamanLaporan Akhir Tugas SiapPutri NurhidayatiBelum ada peringkat
- Terjemahan ADokumen8 halamanTerjemahan ANina SunartiniBelum ada peringkat
- Hospital Management Assesment - Amelia AndrianiDokumen11 halamanHospital Management Assesment - Amelia AndrianiAmelia AndrianiBelum ada peringkat
- PROPOSAL Pengadaan Ruang HD Di Isolasi SeruniDokumen4 halamanPROPOSAL Pengadaan Ruang HD Di Isolasi SeruniendroBelum ada peringkat
- Essay Gadar Dian PratamaDokumen6 halamanEssay Gadar Dian PratamaDian PratamaBelum ada peringkat
- FINAL - Guideline COVID Final + Ref PDFDokumen115 halamanFINAL - Guideline COVID Final + Ref PDFmitraBelum ada peringkat
- TB Masa PandemiDokumen11 halamanTB Masa PandemiReza RezitaBelum ada peringkat
- Jawaban Lidia Sken A BLOK 7Dokumen17 halamanJawaban Lidia Sken A BLOK 7Lidia fransiskaBelum ada peringkat
- Adaptasi PS Kanker Di Era Covid 19Dokumen42 halamanAdaptasi PS Kanker Di Era Covid 19WelasningrumBelum ada peringkat
- Pak Covid-19 UgdDokumen42 halamanPak Covid-19 UgdRestuAnggrainiBelum ada peringkat
- Protokol Penelitian Uji Klinik Ivig Rsup Prof R.D. KandouDokumen24 halamanProtokol Penelitian Uji Klinik Ivig Rsup Prof R.D. KandouAnonymous CKAborxxwBelum ada peringkat
- Pengaruh Terjadinya Isu Dampak Negatif Tentang Rujuk Pasien Covid Ke Rumah SakitDokumen11 halamanPengaruh Terjadinya Isu Dampak Negatif Tentang Rujuk Pasien Covid Ke Rumah SakitLuluKhoiriyahBelum ada peringkat
- P1337420617007 - Fitri Asih - Covid19Dokumen5 halamanP1337420617007 - Fitri Asih - Covid19Gandos AbadiBelum ada peringkat
- Jurnal Sains Dan Kesehatan: Laporan Kasus: Terapi Covid-19 Pada Pasien Dengan Komorbid HipertensiDokumen9 halamanJurnal Sains Dan Kesehatan: Laporan Kasus: Terapi Covid-19 Pada Pasien Dengan Komorbid HipertensiSholBelum ada peringkat
- Manajemen Keperawatan Covid Dan Prone PositionDokumen40 halamanManajemen Keperawatan Covid Dan Prone PositionDhilaBelum ada peringkat
- Makalah Asuhan Keperawatan Pada Covid-19Dokumen14 halamanMakalah Asuhan Keperawatan Pada Covid-19Gita SafitriBelum ada peringkat
- Asuhan Keperawatan Pasien Covid 19 Dengan KomorbidDokumen47 halamanAsuhan Keperawatan Pasien Covid 19 Dengan KomorbidNikoss FaBelum ada peringkat
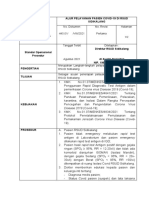
- Alur Pelayanan Pasien CovidDokumen2 halamanAlur Pelayanan Pasien CovidlegersihBelum ada peringkat
- Keperawatan TropisDokumen6 halamanKeperawatan TropismuhalwanBelum ada peringkat
- New Revisi BAB II - Henny Hardiyanty - SNR19214036-1Dokumen43 halamanNew Revisi BAB II - Henny Hardiyanty - SNR19214036-1JuliusAdiNugrahaBelum ada peringkat
- Bab 2Dokumen21 halamanBab 2WP GamingBelum ada peringkat
- Radiologic Aspects of COVID-19 PneumoniaDokumen16 halamanRadiologic Aspects of COVID-19 PneumoniaMuhammad ImamHanafiBelum ada peringkat
- SOP Pelayanan CovidDokumen3 halamanSOP Pelayanan CovidYudi Solehudin100% (3)
- 692-Article Text-4824-1-10-20211222 NADADokumen8 halaman692-Article Text-4824-1-10-20211222 NADAamirul hadiBelum ada peringkat
- Ringkasan - Pengenalan Covid-19Dokumen7 halamanRingkasan - Pengenalan Covid-19Indi EkanantaBelum ada peringkat
- Cme - Sana Ghita Fauziah - Ayugita Nurazizah Tamad - Koas Daring Periodei 6 Juli - 8 Agustus 2020Dokumen21 halamanCme - Sana Ghita Fauziah - Ayugita Nurazizah Tamad - Koas Daring Periodei 6 Juli - 8 Agustus 2020saghita fauziahBelum ada peringkat
- 1 PBDokumen11 halaman1 PBTiffany UsnaBelum ada peringkat
- Coronavirus Covid-19. Membela diri. Cara menghindari penularan. Bagaimana melindungi keluarga dan pekerjaan Anda. Diperbarui edisi keempat.Dari EverandCoronavirus Covid-19. Membela diri. Cara menghindari penularan. Bagaimana melindungi keluarga dan pekerjaan Anda. Diperbarui edisi keempat.Penilaian: 5 dari 5 bintang5/5 (2)
- Borang AgnesDokumen27 halamanBorang Agnesbagus susetioBelum ada peringkat
- WahanaPeriode1 2021portalDokumen75 halamanWahanaPeriode1 2021portalbagus susetioBelum ada peringkat
- Acute Stroke Management in Pandemic Covid JournalDokumen14 halamanAcute Stroke Management in Pandemic Covid Journalbagus susetioBelum ada peringkat
- Review IshipDokumen11 halamanReview IshipHambali Humam0% (2)
- Tugas Referat Galukoma Akut FixDokumen38 halamanTugas Referat Galukoma Akut Fixbagus susetioBelum ada peringkat
- Borang AgnesDokumen27 halamanBorang Agnesbagus susetioBelum ada peringkat
- Keperluan BayiDokumen4 halamanKeperluan Bayibagus susetioBelum ada peringkat
- CV DR BagsDokumen1 halamanCV DR Bagsbagus susetioBelum ada peringkat
- Referat Sindrom Koroner AkutDokumen11 halamanReferat Sindrom Koroner Akutbagus susetioBelum ada peringkat
- CBD IchDokumen24 halamanCBD Ichbagus susetioBelum ada peringkat
- Refrat ACSDokumen21 halamanRefrat ACSbagus susetioBelum ada peringkat
- Refleksi Kasus SilkaDokumen4 halamanRefleksi Kasus Silkabagus susetioBelum ada peringkat
- Artikel Herbal DM Tipe 2Dokumen7 halamanArtikel Herbal DM Tipe 2bagus susetioBelum ada peringkat
- Tugas Referat Galukoma Akut FixDokumen38 halamanTugas Referat Galukoma Akut Fixbagus susetioBelum ada peringkat
- Tugas Referat Galukoma Akut FixDokumen38 halamanTugas Referat Galukoma Akut Fixbagus susetioBelum ada peringkat
- Pptbronkopneumonia 160816152208Dokumen41 halamanPptbronkopneumonia 160816152208Padang Tri handoyoBelum ada peringkat
- CBD KBDokumen12 halamanCBD KBbagus susetioBelum ada peringkat
- OslerTB FixDokumen52 halamanOslerTB Fixbagus susetioBelum ada peringkat
- Refrat SilkaDokumen32 halamanRefrat Silkabagus susetioBelum ada peringkat
- CBD DOTS SilkaDokumen28 halamanCBD DOTS Silkabagus susetioBelum ada peringkat
- Bronkopneumonia RadiologiDokumen34 halamanBronkopneumonia Radiologipoppy_thahir100% (4)
- CBD DOTS SilkaDokumen28 halamanCBD DOTS Silkabagus susetioBelum ada peringkat
- SKABIESDokumen22 halamanSKABIESbagus susetioBelum ada peringkat
- Bab Ii Tinjauan PustakaDokumen22 halamanBab Ii Tinjauan PustakaÜhêh ÜbrütBelum ada peringkat
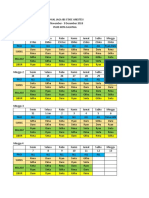
- Jadwal Jaga Ibs Anestesi D.R.G.S.R.Dokumen2 halamanJadwal Jaga Ibs Anestesi D.R.G.S.R.silka reslia riswantoBelum ada peringkat
- Referat Otopsi Virtual 222Dokumen27 halamanReferat Otopsi Virtual 222bagus susetioBelum ada peringkat
- Refrat SilkaDokumen32 halamanRefrat Silkabagus susetioBelum ada peringkat
- Refleksi Kasus IkmDokumen4 halamanRefleksi Kasus Ikmbagus susetioBelum ada peringkat
- Referat Otopsi Virtual 222Dokumen27 halamanReferat Otopsi Virtual 222bagus susetioBelum ada peringkat