Anda mungkin juga menyukai
- Pe EklamsiaTerbaru - DR - Sutoko - 4 11 2022Dokumen98 halamanPe EklamsiaTerbaru - DR - Sutoko - 4 11 2022Chellyani Chantika DamayantiBelum ada peringkat
- Askarani Kamilasari POMR HipertensiDokumen8 halamanAskarani Kamilasari POMR Hipertensifaruq azmiBelum ada peringkat
- HT KronisDokumen17 halamanHT KronisJlo CahyatiBelum ada peringkat
- Preeklampsia EDITDokumen37 halamanPreeklampsia EDITluthfi riski2404Belum ada peringkat
- Lapsus Plasenta PreviaDokumen38 halamanLapsus Plasenta PreviaAvril T WarkeyBelum ada peringkat
- Hipertensi Dalam Kehamilan .Dokumen6 halamanHipertensi Dalam Kehamilan .IrfanBelum ada peringkat
- Laporan Kasus Obgyn FixxDokumen28 halamanLaporan Kasus Obgyn FixxFheysin Permatasari MoyoBelum ada peringkat
- Lapkas HT BMDokumen20 halamanLapkas HT BMFitra HadiBelum ada peringkat
- Crs Prematur KontraksiDokumen9 halamanCrs Prematur KontraksiDita Evita HersafitriBelum ada peringkat
- ppt-Laporan-Kasus 1Dokumen50 halamanppt-Laporan-Kasus 1YuniBelum ada peringkat
- Laporan Kasus HEG DundaDokumen10 halamanLaporan Kasus HEG DundaMiss SugaBelum ada peringkat
- Hipertensi Dalam KehamilanDokumen41 halamanHipertensi Dalam Kehamilansulin ziyatiBelum ada peringkat
- Laporan Kasus 24-02-2020 HEG K31Dokumen19 halamanLaporan Kasus 24-02-2020 HEG K31Tri Ananda Adi PranotoBelum ada peringkat
- Hipertensi GestasionalDokumen11 halamanHipertensi Gestasionalnurbasuki75Belum ada peringkat
- Pelayanan Rujukan Maternal DasarDokumen48 halamanPelayanan Rujukan Maternal DasarSalmaBelum ada peringkat
- Laporan Kasus PEB ISIPDokumen28 halamanLaporan Kasus PEB ISIPRiaGustriaPohan100% (1)
- PPK Hipertensi Pada AnakDokumen12 halamanPPK Hipertensi Pada AnakLisa TreveBelum ada peringkat
- Pre Eklampsia Berat LWPDokumen17 halamanPre Eklampsia Berat LWPAdhi Nugroho LatiefBelum ada peringkat
- Megacolon CongenitalDokumen18 halamanMegacolon CongenitalIrma Dewayanti100% (1)
- POMR 30 Mei 2023Dokumen5 halamanPOMR 30 Mei 2023Anindya FirdausBelum ada peringkat
- Sop Hipertensi Dalam KehamilanDokumen3 halamanSop Hipertensi Dalam KehamilanDila KhairunnisaBelum ada peringkat
- Case Based Discussion - Gagah BrillianDokumen15 halamanCase Based Discussion - Gagah BrillianGagah BrillianBelum ada peringkat
- Laporan Kasus Preeklampsia BeratDokumen32 halamanLaporan Kasus Preeklampsia BeratNabil Ihsan AhmadBelum ada peringkat
- PPK Demam Netropenia 2020 FinalDokumen3 halamanPPK Demam Netropenia 2020 FinalBella Dirk100% (1)
- Lapkas ObgynDokumen46 halamanLapkas ObgynSandrio LahdisaBelum ada peringkat
- Mola HidatidosaDokumen29 halamanMola Hidatidosaselma balafifBelum ada peringkat
- PDF Borang ObgynDokumen13 halamanPDF Borang ObgynGandaBelum ada peringkat
- Ahmad TeguhDokumen2 halamanAhmad Teguhalfaz zamzamiBelum ada peringkat
- PPKDokumen16 halamanPPKhettyBelum ada peringkat
- PPK Demam Netropenia 2020 Final-1Dokumen4 halamanPPK Demam Netropenia 2020 Final-1Bella DirkBelum ada peringkat
- Askep Kehamilan BeresikoDokumen13 halamanAskep Kehamilan BeresikoRatih EkaBelum ada peringkat
- Mini Tryout Obgyn (Asah)Dokumen17 halamanMini Tryout Obgyn (Asah)Koas kompreBelum ada peringkat
- Hipertensi Dalam KehamilanDokumen21 halamanHipertensi Dalam Kehamilannando8396Belum ada peringkat
- Hellp SyndromeDokumen28 halamanHellp SyndromeDiana YanaBelum ada peringkat
- Monre Rsud DR La Palaloi Maros 05 November 2022Dokumen9 halamanMonre Rsud DR La Palaloi Maros 05 November 2022Muhammad SyukurBelum ada peringkat
- Laporan Kasus HapDokumen9 halamanLaporan Kasus HapGunawan Efri SBelum ada peringkat
- PreeklampsiaDokumen30 halamanPreeklampsiaRezki emelliaBelum ada peringkat
- HIPERTENSI DALAM KEHAMILAN - PPT, SEMINARDokumen36 halamanHIPERTENSI DALAM KEHAMILAN - PPT, SEMINARzaroziBelum ada peringkat
- Hipertensi AnakDokumen36 halamanHipertensi AnakGabriela WatilayBelum ada peringkat
- Borang InternaDokumen23 halamanBorang Internafadhillah islamyahprBelum ada peringkat
- Monre Rsud DR La Palaloi Maros 05 November 2022Dokumen9 halamanMonre Rsud DR La Palaloi Maros 05 November 2022Muhammad SyukurBelum ada peringkat
- Laporan Kasus Hipertensi GestasionalDokumen32 halamanLaporan Kasus Hipertensi GestasionalFuchsia Zein100% (1)
- CaseWS HipertensiemergensiDokumen14 halamanCaseWS HipertensiemergensiRizky NurindraBelum ada peringkat
- CaseDokumen30 halamanCaseDavid TurnerBelum ada peringkat
- PreeklampsiaDokumen44 halamanPreeklampsiaresiBelum ada peringkat
- GABUNGANDokumen8 halamanGABUNGANTelat GamingBelum ada peringkat
- Morning Report Rs Alfatah Agustus FixDokumen42 halamanMorning Report Rs Alfatah Agustus FixKoas Neuro UnpattiBelum ada peringkat
- SK 2: Risiko Kehamilan: Wednesday, September 14, 2022 6:41 AMDokumen4 halamanSK 2: Risiko Kehamilan: Wednesday, September 14, 2022 6:41 AMDEWI MEIRA ROSABelum ada peringkat
- HipertensiDokumen64 halamanHipertensialmahyra apotekBelum ada peringkat
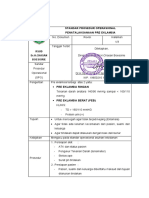
- SPO Pre EklampsiaDokumen4 halamanSPO Pre Eklampsiaruang obstetriBelum ada peringkat
- Referat Hipertensi AnakDokumen23 halamanReferat Hipertensi AnakMichael Spica RampangileiBelum ada peringkat
- Pre Eklamsia Berat: Dria Nur Fathan 13711037Dokumen34 halamanPre Eklamsia Berat: Dria Nur Fathan 13711037Auliya AndiBelum ada peringkat
- Kegawatdaruratan ObstetriDokumen80 halamanKegawatdaruratan Obstetriniahsusianti79Belum ada peringkat
- Bab 2 CindyDokumen11 halamanBab 2 CindyDhian Tyara SariBelum ada peringkat
- HIPERTENSI Dalam KEHAMILANDokumen2 halamanHIPERTENSI Dalam KEHAMILANDevanti EkaBelum ada peringkat
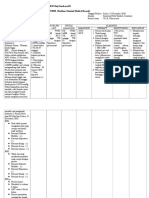
- WM-Diagnosis PEB Atipikal-WMDokumen40 halamanWM-Diagnosis PEB Atipikal-WMasoly giovanoBelum ada peringkat
- Preeklamsia BeratDokumen37 halamanPreeklamsia Beratdedyz_11075957Belum ada peringkat
- Laporan Kasus Slide Mola Hidatidosa NiningDokumen28 halamanLaporan Kasus Slide Mola Hidatidosa NiningArini HadipatyBelum ada peringkat
- Preeklamsia BeratDokumen37 halamanPreeklamsia BeratyuliBelum ada peringkat
- Makalah Kelompok 3 Kelas 1a Callista Roy - CompressDokumen20 halamanMakalah Kelompok 3 Kelas 1a Callista Roy - Compresssri faidahBelum ada peringkat
- Terapi MemaafkanDokumen40 halamanTerapi Memaafkansri faidahBelum ada peringkat
- PDF Laporan Pendahuluan Nefrolitiasis - CompressDokumen28 halamanPDF Laporan Pendahuluan Nefrolitiasis - Compresssri faidahBelum ada peringkat
- Modul Petunjuk Praktikum Keperawatan Medikal Bedah 2Dokumen28 halamanModul Petunjuk Praktikum Keperawatan Medikal Bedah 2sri faidahBelum ada peringkat
- Terapi PemaafanDokumen28 halamanTerapi Pemaafansri faidahBelum ada peringkat
- LP SerotinusDokumen20 halamanLP Serotinussri faidahBelum ada peringkat
- KLP 2 Kep Komunitas.2Dokumen50 halamanKLP 2 Kep Komunitas.2sri faidahBelum ada peringkat
- Demam Berdarah Dengue Pada AnakDokumen27 halamanDemam Berdarah Dengue Pada Anaksri faidahBelum ada peringkat
- Kep Komunitas Bu Wied-1Dokumen17 halamanKep Komunitas Bu Wied-1sri faidahBelum ada peringkat
- Laporan Pendahuluan Post PartumDokumen19 halamanLaporan Pendahuluan Post Partumsri faidahBelum ada peringkat
- Sistem ImunDokumen10 halamanSistem Imunsri faidahBelum ada peringkat
- Akhlaq Ortu KPD AnakDokumen26 halamanAkhlaq Ortu KPD Anaksri faidahBelum ada peringkat
- Kebutuhan Dasar Post PartumDokumen18 halamanKebutuhan Dasar Post Partumsri faidahBelum ada peringkat
- Sri Faidah: Tentang SayaDokumen1 halamanSri Faidah: Tentang Sayasri faidahBelum ada peringkat
- Satuan Acara Penyuluhan FixDokumen22 halamanSatuan Acara Penyuluhan Fixsri faidahBelum ada peringkat
- Buku Panduan Praktek Maternitas S1 Kep Tingkat 2 Tahun 2022Dokumen31 halamanBuku Panduan Praktek Maternitas S1 Kep Tingkat 2 Tahun 2022sri faidahBelum ada peringkat
- Persiapan Kehamilan BerkualitasDokumen11 halamanPersiapan Kehamilan Berkualitassri faidahBelum ada peringkat
- Askep DM KronisDokumen14 halamanAskep DM Kronissri faidahBelum ada peringkat
- 4.bab 1Dokumen4 halaman4.bab 1sri faidahBelum ada peringkat
- Nindra LP SNDokumen7 halamanNindra LP SNsri faidahBelum ada peringkat
- HAMBATAN KOMUNIKASI PAK RULLY KELOMPOK 6 NewwDokumen23 halamanHAMBATAN KOMUNIKASI PAK RULLY KELOMPOK 6 Newwsri faidahBelum ada peringkat
- Kel 1. Makalah Anfis OtakDokumen11 halamanKel 1. Makalah Anfis Otaksri faidahBelum ada peringkat
- SP Siska Safitri Bu TrimeliaDokumen13 halamanSP Siska Safitri Bu Trimeliasri faidahBelum ada peringkat
- Toaz - Info Laporan Ca Renal Anggrek PR - DikonversiDokumen20 halamanToaz - Info Laporan Ca Renal Anggrek PR - Dikonversisri faidahBelum ada peringkat
- Materi Pembekalan Skillab Sistem EndokrinDokumen4 halamanMateri Pembekalan Skillab Sistem Endokrinsri faidahBelum ada peringkat
- Tugas Kel 2 (Idk 2)Dokumen14 halamanTugas Kel 2 (Idk 2)sri faidahBelum ada peringkat