0% menganggap dokumen ini bermanfaat (0 suara)
147 tayangan30 halamanIUGR - Dr. ART
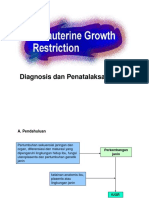
Dokumen tersebut membahas klasifikasi IUGR berdasarkan stadium berdasarkan gejala klinis, umur onset, dan hasil pemeriksaan Doppler. Ada 4 stadium IUGR yang dijelaskan berdasarkan tingkat keparahan gangguan plasenta dan risiko deteriorasi janin, beserta rekomendasi penanganan untuk masing-masing stadium. Stadium lebih lanjut menandakan gangguan plasenta yang lebih parah dan risiko kematian janin atau kelainan yang lebih besar.
Diunggah oleh
Bernas Arion NapitupuluHak Cipta
© © All Rights Reserved
Kami menangani hak cipta konten dengan serius. Jika Anda merasa konten ini milik Anda, ajukan klaim di sini.
Format Tersedia
Unduh sebagai PPTX, PDF, TXT atau baca online di Scribd
0% menganggap dokumen ini bermanfaat (0 suara)
147 tayangan30 halamanIUGR - Dr. ART
Dokumen tersebut membahas klasifikasi IUGR berdasarkan stadium berdasarkan gejala klinis, umur onset, dan hasil pemeriksaan Doppler. Ada 4 stadium IUGR yang dijelaskan berdasarkan tingkat keparahan gangguan plasenta dan risiko deteriorasi janin, beserta rekomendasi penanganan untuk masing-masing stadium. Stadium lebih lanjut menandakan gangguan plasenta yang lebih parah dan risiko kematian janin atau kelainan yang lebih besar.
Diunggah oleh
Bernas Arion NapitupuluHak Cipta
© © All Rights Reserved
Kami menangani hak cipta konten dengan serius. Jika Anda merasa konten ini milik Anda, ajukan klaim di sini.
Format Tersedia
Unduh sebagai PPTX, PDF, TXT atau baca online di Scribd