Anda mungkin juga menyukai
- Rehidrasi CairanDokumen54 halamanRehidrasi CairanKennyBelum ada peringkat
- Presentasi 2 Keseimbangan Cairan Dan ElektrolitDokumen54 halamanPresentasi 2 Keseimbangan Cairan Dan ElektrolitNur Ismaniar TahirBelum ada peringkat
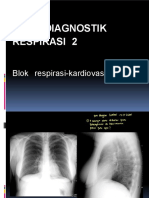
- RadiologiDokumen130 halamanRadiologiFiqri NovianBelum ada peringkat
- Terapi Cairan Dan ElektrolitDokumen77 halamanTerapi Cairan Dan ElektrolitarvianamearsaBelum ada peringkat
- Terapi CairanDokumen64 halamanTerapi Cairanravannofanizza100% (2)
- DEHIDRASIDokumen22 halamanDEHIDRASITridiaPutraGunantaBelum ada peringkat
- Biokimia Keseimbangan Asam BasaDokumen39 halamanBiokimia Keseimbangan Asam BasaPisthaPrima'Pistha'0% (1)
- Radio NeoplasmatikDokumen133 halamanRadio NeoplasmatikFiqri Novian100% (1)
- Fluid and ElectrolytesDokumen97 halamanFluid and ElectrolytesMiftahul KhasanahBelum ada peringkat
- Kadar Natrium Dalam DarahDokumen32 halamanKadar Natrium Dalam DarahhendrajokerBelum ada peringkat
- TUGAS Gangguan-ElektrolitDokumen33 halamanTUGAS Gangguan-ElektrolitEka RendyBelum ada peringkat
- Terapi Cairan Dan Asam BasaDokumen58 halamanTerapi Cairan Dan Asam BasadrlazyboyBelum ada peringkat
- Diuretik NewDokumen24 halamanDiuretik NewIthyn Mudha MakindBelum ada peringkat
- REFERAT - Gangguan Elektrolit (Fix)Dokumen28 halamanREFERAT - Gangguan Elektrolit (Fix)Flavia Angel SatopohBelum ada peringkat
- Gangguan Elektrolit NatriumDokumen18 halamanGangguan Elektrolit NatriumYoan PratamaBelum ada peringkat
- Terapi Cairan APHiDokumen61 halamanTerapi Cairan APHiMagfira GuntataBelum ada peringkat
- Keseimbangan ElektrolitDokumen28 halamanKeseimbangan ElektrolitAgatha Rhana AveonitaBelum ada peringkat
- Cairan Tubuh 21Dokumen76 halamanCairan Tubuh 21Virgiana ListiantiBelum ada peringkat
- TUGAS IBD (2) Resume Materi - Cinta Meilika - 222040 - 1B - S1Dokumen28 halamanTUGAS IBD (2) Resume Materi - Cinta Meilika - 222040 - 1B - S1Cinta MeilikaBelum ada peringkat
- KEBUTUHAN CAIRAN & ELEKTROLIT GO HRDokumen38 halamanKEBUTUHAN CAIRAN & ELEKTROLIT GO HRichaniisaazBelum ada peringkat
- CAIRANDokumen57 halamanCAIRANFitriBelum ada peringkat
- Cairan Tubuh BLOK IKD 2Dokumen30 halamanCairan Tubuh BLOK IKD 2Abdul Malik FajriBelum ada peringkat
- Bimbingan-Terapi CairanDokumen49 halamanBimbingan-Terapi CairanmiazaraBelum ada peringkat
- Hypertonic Sodium Lactate SolutionDokumen45 halamanHypertonic Sodium Lactate SolutionDiyos SupriantoBelum ada peringkat
- Asam BasaDokumen29 halamanAsam BasaMohammadAriefKurniawanBelum ada peringkat
- GUS1-K22 (PPT ST 19) Diagnosis Gangguan Keseimbangan Air, Elektrolit Dan Asam-BasaDokumen34 halamanGUS1-K22 (PPT ST 19) Diagnosis Gangguan Keseimbangan Air, Elektrolit Dan Asam-BasaMarieta RitongaBelum ada peringkat
- Cairan ElektrolitDokumen43 halamanCairan ElektrolitHerwin Sopiona TumanggorBelum ada peringkat
- Terapi Nutrisi Dan Cairan 1588538925Dokumen84 halamanTerapi Nutrisi Dan Cairan 1588538925Pransiska oktavianiBelum ada peringkat
- Cairan Tubuh - SismadiDokumen29 halamanCairan Tubuh - SismadiKeperawatan RSUD CibinongBelum ada peringkat
- Tatalaksana Pemberian Cairan Pada Anak - Welda Daud (19.128)Dokumen21 halamanTatalaksana Pemberian Cairan Pada Anak - Welda Daud (19.128)Shira YukiBelum ada peringkat
- Konsep Kebutuhan Asam BasaDokumen28 halamanKonsep Kebutuhan Asam BasaAldinBelum ada peringkat
- Cairan Dan ElektrolitDokumen36 halamanCairan Dan Elektrolitrany permata sariBelum ada peringkat
- Pertemuan 15 KimiaklinikDokumen46 halamanPertemuan 15 KimiaklinikMuhammad AndreBelum ada peringkat
- DehidrasiDokumen34 halamanDehidrasitofan widyaBelum ada peringkat
- Terapi FluidaDokumen41 halamanTerapi FluidaGalih Fernando PradanaBelum ada peringkat
- Keseimbangan Cairan Dan Asam BasaDokumen43 halamanKeseimbangan Cairan Dan Asam BasaIm IrnBelum ada peringkat
- Metabolisme Air Dan ElektrolitDokumen30 halamanMetabolisme Air Dan Elektrolitviviyanti znBelum ada peringkat
- Cairan Tubuh N AsbasaDokumen29 halamanCairan Tubuh N AsbasaCHoy RobluccyBelum ada peringkat
- Gus K-20 GGN Keseimbangan Air, Elektrolit & As BasaDokumen34 halamanGus K-20 GGN Keseimbangan Air, Elektrolit & As BasaHanidya FazwatBelum ada peringkat
- 2 Keseimbangan Cairan Dan Elektrolit 1Dokumen35 halaman2 Keseimbangan Cairan Dan Elektrolit 1Ligia OSuandiBelum ada peringkat
- Cairan Tubuh + Asam BasaDokumen29 halamanCairan Tubuh + Asam BasaAsgar UsmanBelum ada peringkat
- Kelompok 6 GANGGUAN ELEKTROLIT MFK 2018 + JawabanDokumen91 halamanKelompok 6 GANGGUAN ELEKTROLIT MFK 2018 + JawabansisrinovritaBelum ada peringkat
- Biokimia PernapasanDokumen11 halamanBiokimia PernapasanAkhmad Maulana KhaqBelum ada peringkat
- Gangguan Kebutuhan Cairan Patologis KMB 1 2019Dokumen28 halamanGangguan Kebutuhan Cairan Patologis KMB 1 2019Andi MutmainnahBelum ada peringkat
- Cairan Dan ElektrolitDokumen31 halamanCairan Dan ElektrolitTri RachmadijantoBelum ada peringkat
- Resusitasi Cairan Izma DaudDokumen61 halamanResusitasi Cairan Izma DaudAtika Yulan OppoBelum ada peringkat
- Idk Cairan TubuhDokumen31 halamanIdk Cairan TubuhRaesa TartillaBelum ada peringkat
- Interpretasi Asam BasaDokumen24 halamanInterpretasi Asam BasaA BBelum ada peringkat
- PATOFISIOLOGI EdemaDokumen6 halamanPATOFISIOLOGI EdemaRandhya WijayaBelum ada peringkat
- GG - Cairan & ElektrolitDokumen59 halamanGG - Cairan & ElektrolitCatur AsmaraniBelum ada peringkat
- Konsep Cairan, El, As-BsDokumen75 halamanKonsep Cairan, El, As-BsgitaqBelum ada peringkat
- Keseimbangan CairanDokumen32 halamanKeseimbangan Cairanandre setyawanBelum ada peringkat
- Jafri - Keseimbangan, Cairan Dan Asam BasaDokumen3 halamanJafri - Keseimbangan, Cairan Dan Asam BasaannisaBelum ada peringkat
- Terapi Cairan Pada Tatalaksana Dehidrasi Dan Syok Hipovolemik Serta Perdarahan - AnestesiDokumen53 halamanTerapi Cairan Pada Tatalaksana Dehidrasi Dan Syok Hipovolemik Serta Perdarahan - AnestesiPratikaLawrenceSasubeBelum ada peringkat
- 3665 - PPT DR Lucy FixDokumen45 halaman3665 - PPT DR Lucy FixGeryAldilatamaBelum ada peringkat
- Referat Gangguan ElektrolitDokumen22 halamanReferat Gangguan ElektrolitkartinisBelum ada peringkat
- Keseimbangan Cairan Dan Elektrolit - CompressedDokumen40 halamanKeseimbangan Cairan Dan Elektrolit - CompressedSukses TinggiBelum ada peringkat
- Tentiran Asam Basa - NasyaDokumen16 halamanTentiran Asam Basa - NasyaAA Ngr Oka ParamawangsaBelum ada peringkat
- Bab Sistem Ekskresi Manusia Lengkap 111231073514 Phpapp02Dokumen30 halamanBab Sistem Ekskresi Manusia Lengkap 111231073514 Phpapp02Aten Putrii13Belum ada peringkat
- Keseimbangan Asam BasaDokumen29 halamanKeseimbangan Asam BasaTA 76nBelum ada peringkat
- JADWAL DINAS COASS 29 Mei - 4 Juni 2023Dokumen4 halamanJADWAL DINAS COASS 29 Mei - 4 Juni 2023Fiqri NovianBelum ada peringkat
- Rational Use of MedicineDokumen54 halamanRational Use of MedicineFiqri NovianBelum ada peringkat
- BiokimiaDokumen19 halamanBiokimiaFiqri NovianBelum ada peringkat
- DIGESTIVEDokumen16 halamanDIGESTIVEFiqri NovianBelum ada peringkat
- JADWAL DINAS COASS 5 - 11 Juni 2023Dokumen4 halamanJADWAL DINAS COASS 5 - 11 Juni 2023Fiqri NovianBelum ada peringkat
- Anatomi FisiologiDokumen8 halamanAnatomi FisiologiFiqri NovianBelum ada peringkat
- Keseimbangan Asam Basa, 2016Dokumen53 halamanKeseimbangan Asam Basa, 2016Fiqri NovianBelum ada peringkat
- Proposal Ramadhan AMSA-Untad 2021Dokumen8 halamanProposal Ramadhan AMSA-Untad 2021Fiqri NovianBelum ada peringkat
- BiokimDokumen6 halamanBiokimFiqri NovianBelum ada peringkat
- Silabus SKDokumen2 halamanSilabus SKFiqri NovianBelum ada peringkat
- Radiologi NeuromuskuloDokumen126 halamanRadiologi NeuromuskuloFiqri Novian100% (1)
- Radio 2Dokumen79 halamanRadio 2Fiqri NovianBelum ada peringkat
- Principles of PharmacotherapyDokumen40 halamanPrinciples of PharmacotherapyFiqri NovianBelum ada peringkat
- Moh Fiqri Novian - N11122043 - Refarat - PneumoperitoneumDokumen26 halamanMoh Fiqri Novian - N11122043 - Refarat - PneumoperitoneumFiqri NovianBelum ada peringkat
- Anatomi F18RADokumen10 halamanAnatomi F18RAFiqri NovianBelum ada peringkat
- Silabus MCC MuskuloskeletalDokumen5 halamanSilabus MCC MuskuloskeletalFiqri NovianBelum ada peringkat
- Moh. Fiqri Novian Affandy - Expertise RadiologiDokumen12 halamanMoh. Fiqri Novian Affandy - Expertise RadiologiFiqri NovianBelum ada peringkat
- Dasar Urologi - FMDokumen101 halamanDasar Urologi - FMFiqri NovianBelum ada peringkat
- Untitled NotebookDokumen3 halamanUntitled NotebookFiqri NovianBelum ada peringkat
- Dasar Radiologi MuskularDokumen50 halamanDasar Radiologi MuskularFiqri NovianBelum ada peringkat
- 866-Article Text-3776-1-10-20191217Dokumen2 halaman866-Article Text-3776-1-10-20191217Fiqri NovianBelum ada peringkat
- Radiologi PencernaanDokumen92 halamanRadiologi PencernaanFiqri NovianBelum ada peringkat
- Pneumoperitoneum RashifDokumen20 halamanPneumoperitoneum RashifFiqri NovianBelum ada peringkat
- Jenis Formula Resep DokterDokumen3 halamanJenis Formula Resep DokterFiqri NovianBelum ada peringkat
- Kasus 4.en - IdDokumen4 halamanKasus 4.en - IdFiqri NovianBelum ada peringkat
- ANGIOGRAFIDokumen13 halamanANGIOGRAFIFiqri NovianBelum ada peringkat
- Tanner2018 en IdDokumen18 halamanTanner2018 en IdFiqri NovianBelum ada peringkat
- Kasus 3.en - IdDokumen5 halamanKasus 3.en - IdFiqri NovianBelum ada peringkat