Anda mungkin juga menyukai
- StrokeDokumen41 halamanStrokePutri GintingBelum ada peringkat
- StrokeDokumen47 halamanStrokesri wula moniBelum ada peringkat
- Presentasi Stroke HISFARSI - AcehDokumen72 halamanPresentasi Stroke HISFARSI - Acehbobobo22Belum ada peringkat
- PLENO Pemicu 6 SarafDokumen40 halamanPLENO Pemicu 6 SarafIca BatalipuBelum ada peringkat
- Kuliah 8. Lumpuh Separuh TubuhDokumen32 halamanKuliah 8. Lumpuh Separuh TubuhanggaBelum ada peringkat
- Kuliah CVD Modul NeuroDokumen72 halamanKuliah CVD Modul NeuroZIKRA APRIANI -Belum ada peringkat
- Referat StrokeDokumen50 halamanReferat StrokeIzzam QalbieBelum ada peringkat
- Materi 9 SYOK & RESUSITASI CAIRAN - 2014Dokumen18 halamanMateri 9 SYOK & RESUSITASI CAIRAN - 2014Safira WidyatamiBelum ada peringkat
- StrokeDokumen50 halamanStrokeNurul AmaliaBelum ada peringkat
- (Dr. Verbty, SPS) CVDDokumen92 halaman(Dr. Verbty, SPS) CVDAlfian DaudBelum ada peringkat
- KP 11 Stroke IskemikDokumen40 halamanKP 11 Stroke IskemikvebblyBelum ada peringkat
- Stroke IskemikDokumen38 halamanStroke IskemikBonitavanyBelum ada peringkat
- NeurovascularDokumen34 halamanNeurovascularviraBelum ada peringkat
- Cedera Kepala BeratDokumen61 halamanCedera Kepala BeratTrie SugiartiBelum ada peringkat
- Sindrom Koroner AkutDokumen39 halamanSindrom Koroner AkutSelly Yuliana IndrianiBelum ada peringkat
- SyokDokumen26 halamanSyokAnonymous iTstegX2Belum ada peringkat
- ShockDokumen39 halamanShockAbdelrahman M. AlnweiriBelum ada peringkat
- Kegawatdaruratan JantungDokumen109 halamanKegawatdaruratan JantungMuhammad GilangBelum ada peringkat
- Stroke Iskemik 1Dokumen38 halamanStroke Iskemik 1Mohammad BudiBelum ada peringkat
- Simulasi Stroke Nur SabrinaDokumen20 halamanSimulasi Stroke Nur SabrinaBochand CoolBelum ada peringkat
- Lapsus Internsip - NHSDokumen88 halamanLapsus Internsip - NHSMuhammad Fahry AladjaiBelum ada peringkat
- Askep MCIDokumen5 halamanAskep MCIRizka Rahma AmbarwatiBelum ada peringkat
- Gangguan Sirkulasi SyokDokumen40 halamanGangguan Sirkulasi SyokFatmawati RidwanBelum ada peringkat
- StrokeDokumen26 halamanStrokeKevin Yoshua PadangBelum ada peringkat
- Manajemen Kedaruratan Pada StrokeDokumen46 halamanManajemen Kedaruratan Pada StrokeSlamet PonediBelum ada peringkat
- StemiDokumen72 halamanStemiatika rozaliaBelum ada peringkat
- Askep HematologiDokumen45 halamanAskep HematologiTriani HeriyantyBelum ada peringkat
- Stroke CoasDokumen68 halamanStroke CoasFini AndrianiBelum ada peringkat
- Rehabilitasi JantungDokumen54 halamanRehabilitasi Jantung21701101047 Laksmita AnggaraniBelum ada peringkat
- Dr. APP - Manajemen Syok Untuk Perawat - 2017Dokumen36 halamanDr. APP - Manajemen Syok Untuk Perawat - 2017keriatunBelum ada peringkat
- Buku Bahan Ajar Keperawatan Gawat Darurat Dan KritisDokumen111 halamanBuku Bahan Ajar Keperawatan Gawat Darurat Dan KritisPutri CantikBelum ada peringkat
- Stroke Gen NewDokumen28 halamanStroke Gen Newuwuwu yeahBelum ada peringkat
- LP Icvcu StemiDokumen15 halamanLP Icvcu StemiSettiyana NBelum ada peringkat
- LP StemiDokumen19 halamanLP StemiRicky Arya AdinataBelum ada peringkat
- Presentasi PTM PJPDDokumen39 halamanPresentasi PTM PJPDobie wardanaBelum ada peringkat
- STROKEDokumen30 halamanSTROKEsisva nesaBelum ada peringkat
- Syok Pada AnakDokumen70 halamanSyok Pada AnaklisyaBelum ada peringkat
- Materi Stroke Dr. GomgomDokumen32 halamanMateri Stroke Dr. GomgomCoco ChanelBelum ada peringkat
- PENATALAKSANAAN SYOK PADA ANAK-dewiDokumen53 halamanPENATALAKSANAAN SYOK PADA ANAK-dewiIrenaBelum ada peringkat
- Resusitasi Cairan HMMDokumen33 halamanResusitasi Cairan HMMandi ananBelum ada peringkat
- PADDokumen25 halamanPADNada Rizki HanifahBelum ada peringkat
- 3 AtherotrombosisDokumen45 halaman3 AtherotrombosisYuliet Iman MegaBelum ada peringkat
- Presentasi Pencegahan Penyakit Jantung Koroner HWWDokumen26 halamanPresentasi Pencegahan Penyakit Jantung Koroner HWWfkBelum ada peringkat
- Penyakit Jantung Koroner: Darmawaty Rauf, SP - PK (K) Departemen Patologi Klinik FK UnhasDokumen30 halamanPenyakit Jantung Koroner: Darmawaty Rauf, SP - PK (K) Departemen Patologi Klinik FK UnhasnandaameliaBelum ada peringkat
- ANLS 2011 Kegawatdaruratan StrokeDokumen56 halamanANLS 2011 Kegawatdaruratan StrokeelaBelum ada peringkat
- Cerebrovascular Disease CVD StrokeDokumen75 halamanCerebrovascular Disease CVD StrokeK widyantaraBelum ada peringkat
- Asuhan Keperawatan Klien DG CVD - k3Dokumen61 halamanAsuhan Keperawatan Klien DG CVD - k3Mam RBelum ada peringkat
- Dr. Starry H. Rampengan - Syok Kardiogenik Starry PPT April 2012Dokumen86 halamanDr. Starry H. Rampengan - Syok Kardiogenik Starry PPT April 2012muchlis syahputraBelum ada peringkat
- Icu LP StemiDokumen19 halamanIcu LP StemiMuhamad YusufBelum ada peringkat
- Stemi InferiorDokumen28 halamanStemi InferiorkhalifarahmaniBelum ada peringkat
- LP Dan LK STEMI - B2019001 - Sucita AlifadindahDokumen32 halamanLP Dan LK STEMI - B2019001 - Sucita AlifadindahSucita AliBelum ada peringkat
- Laporan Kasus Cva IchDokumen37 halamanLaporan Kasus Cva IchAndarini NurvikasariBelum ada peringkat
- ReferatDokumen27 halamanReferatathiya nadifaBelum ada peringkat
- Slide InfarkDokumen45 halamanSlide InfarkMuhammad FaisalBelum ada peringkat
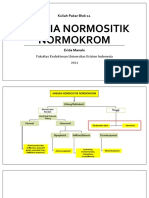
- Anemia Normositik NormokromDokumen52 halamanAnemia Normositik NormokromOrflimeEmmyBelum ada peringkat
- Anemia Normositik NormokromDokumen52 halamanAnemia Normositik NormokromEsaBelum ada peringkat
- Kolesterol 1 5Dokumen5 halamanKolesterol 1 5PersonaliacBelum ada peringkat
- LP Stemi - MappingDokumen3 halamanLP Stemi - MappingSyifa Hasna NadiaBelum ada peringkat
- Komplikasi HipertensiDokumen26 halamanKomplikasi HipertensiLia MukadarBelum ada peringkat
- Lenny RefaratDokumen35 halamanLenny RefaratLennYBelum ada peringkat
- Leaflet KPSPDokumen2 halamanLeaflet KPSPLennYBelum ada peringkat
- Laporan Kasus - Mariani A. MangkutDokumen21 halamanLaporan Kasus - Mariani A. MangkutLennYBelum ada peringkat
- IleusDokumen34 halamanIleusLennYBelum ada peringkat
- Biodata Stase BedahDokumen16 halamanBiodata Stase BedahLennYBelum ada peringkat
- Jurnal Psikiatri Lenny Tri SelvianiDokumen21 halamanJurnal Psikiatri Lenny Tri SelvianiLennYBelum ada peringkat
- Lenny Tri Selviani PPT Jurnal ACLDokumen16 halamanLenny Tri Selviani PPT Jurnal ACLLennYBelum ada peringkat