Anda mungkin juga menyukai
- Penyakit Mata KeringDokumen30 halamanPenyakit Mata KeringdevitaafriskaBelum ada peringkat
- OPTIMALISASI DRY EYEDokumen11 halamanOPTIMALISASI DRY EYEDebby MarianeBelum ada peringkat
- Kerato-Konjungtivitis SiccaDokumen5 halamanKerato-Konjungtivitis SiccaNiki Ayu RezeqiBelum ada peringkat
- Dry Eye SyndromeDokumen7 halamanDry Eye SyndromeniagithaBelum ada peringkat
- Bahan LP FrostbiteDokumen8 halamanBahan LP FrostbiteZakiyah Darajat SulaemanBelum ada peringkat
- Responsi Skabies Dan MHDokumen13 halamanResponsi Skabies Dan MHangelaBelum ada peringkat
- Laporan Kasus 2:glaukoma:astidyaDokumen15 halamanLaporan Kasus 2:glaukoma:astidyaAstidya MirantiBelum ada peringkat
- Tatalaksana DistosiaDokumen2 halamanTatalaksana DistosiaJerrod WilsonBelum ada peringkat
- NotulensiDokumen3 halamanNotulensiFaradela RFBelum ada peringkat
- Makalah Field Study Kelompok 14Dokumen51 halamanMakalah Field Study Kelompok 14Rachman ⎝⏠⏝⏠⎠ BuyungBelum ada peringkat
- Anamnesis Dan Pemeriksaan PsikiatriDokumen11 halamanAnamnesis Dan Pemeriksaan Psikiatriroasted chickenBelum ada peringkat
- Persalinan HisDokumen7 halamanPersalinan HisdicipoknogoBelum ada peringkat
- Tumor UrogenitalDokumen28 halamanTumor UrogenitalKhansa Hanifah MutiaBelum ada peringkat
- Manajemen Dan Rujukan Perdarahan Postpartum Dalam Upaya Penurunan Morbiditas Mortalitas Maternal CompressDokumen10 halamanManajemen Dan Rujukan Perdarahan Postpartum Dalam Upaya Penurunan Morbiditas Mortalitas Maternal CompressalisyaBelum ada peringkat
- Leprosy, Kusta, Morbus Hansen by Dr. Karla Duha Complete VersionDokumen64 halamanLeprosy, Kusta, Morbus Hansen by Dr. Karla Duha Complete VersionKarla DuhaBelum ada peringkat
- Daftar PertanyaanDokumen2 halamanDaftar Pertanyaandewi susilawatiBelum ada peringkat
- Psikofarmaka Obat JiwaDokumen44 halamanPsikofarmaka Obat JiwaNuri FebrianiBelum ada peringkat
- ILMUJIWADokumen3 halamanILMUJIWAMuhammad Yusuf ArrozhiBelum ada peringkat
- MIOPIA RINGANDokumen23 halamanMIOPIA RINGANAlfadea Irbah APBelum ada peringkat
- Pemeriksaan PendengaranDokumen3 halamanPemeriksaan PendengaranAn'umillah Arini ZidnaBelum ada peringkat
- Lepra YudhaDokumen7 halamanLepra YudhayoolinBelum ada peringkat
- MKDKIDokumen14 halamanMKDKIFabian SmithBelum ada peringkat
- CASE REPORT KONJUNGTIVITIS GiriDokumen23 halamanCASE REPORT KONJUNGTIVITIS GiriGiri Mahesa Putra ZatnikaBelum ada peringkat
- Herpes Zoster OftalmikusDokumen7 halamanHerpes Zoster OftalmikusZikra Alfa SaniBelum ada peringkat
- BV_Kandidiasis_ChlamydiaDokumen2 halamanBV_Kandidiasis_ChlamydiaegiflaydiaBelum ada peringkat
- Referat CA VulvaDokumen27 halamanReferat CA Vulvatamara hanna bocanBelum ada peringkat
- Referat RadiologiDokumen39 halamanReferat RadiologiRooy BatkormbawaBelum ada peringkat
- Evaluasi Program Pengendalian Tuberkulosis di Puskesmas Teladan Medan Tahun 2016Dokumen69 halamanEvaluasi Program Pengendalian Tuberkulosis di Puskesmas Teladan Medan Tahun 2016Muhammad FajriBelum ada peringkat
- NotulenBimbinganEEDDokumen5 halamanNotulenBimbinganEEDIriawan Indra PutraBelum ada peringkat
- Referat Sistem Lakrimal Dan KelainannyaDokumen33 halamanReferat Sistem Lakrimal Dan KelainannyamutiaraptrcBelum ada peringkat
- 01 Rangkuman Parkinson DiseaseDokumen5 halaman01 Rangkuman Parkinson DiseaseFiska Praktika WidyawibowoBelum ada peringkat
- SOAL SULIT MATA BLOK 3.3 MahasiswaDokumen6 halamanSOAL SULIT MATA BLOK 3.3 MahasiswaronaaBelum ada peringkat
- Catatan Koas UrologyDokumen11 halamanCatatan Koas UrologyalfianfirdausBelum ada peringkat
- AntihistaminDokumen9 halamanAntihistaminCheni Pathiesvika UntajanaBelum ada peringkat
- DETEKSI PENYAKIT PARUDokumen8 halamanDETEKSI PENYAKIT PARUGharba AnggaraBelum ada peringkat
- Farmakologi UterotonikaDokumen34 halamanFarmakologi Uterotonikaanang kurniawanBelum ada peringkat
- DRY EYESDokumen8 halamanDRY EYESLiona ChristinaBelum ada peringkat
- Sudden DeathDokumen58 halamanSudden DeathRirin WahyuniBelum ada peringkat
- Carotico Covernosus FistulaDokumen22 halamanCarotico Covernosus FistulaDudiBelum ada peringkat
- Penyakit ParkinsonDokumen3 halamanPenyakit ParkinsonAnonymous ENdoGXxsnBelum ada peringkat
- Obat Anti JamurDokumen52 halamanObat Anti JamurHery AkbarBelum ada peringkat
- Pemeriksaan PsikiatriDokumen7 halamanPemeriksaan PsikiatriIsmail Satrio WibowoBelum ada peringkat
- Laporan KasusDokumen27 halamanLaporan KasusZaharatulNurdinBelum ada peringkat
- FERTY6Dokumen72 halamanFERTY6DRIABelum ada peringkat
- Herper Zoster OphthalmicusDokumen26 halamanHerper Zoster OphthalmicusRahmi HayatiBelum ada peringkat
- Psikodinamika DepresiDokumen56 halamanPsikodinamika Depresiamy mulia rizqiBelum ada peringkat
- Makalah Presus IKKDokumen39 halamanMakalah Presus IKKKhaulla KarimaBelum ada peringkat
- Catatan Ujian ObgynDokumen13 halamanCatatan Ujian ObgynDiana WulandariBelum ada peringkat
- Laporan Kasus-PrurigoDokumen30 halamanLaporan Kasus-PrurigoNur'aini FatmawatiBelum ada peringkat
- Hernia Nucleus Pulposus (HNPDokumen26 halamanHernia Nucleus Pulposus (HNPjesika ita niomiBelum ada peringkat
- SUDDEN DEATHDokumen46 halamanSUDDEN DEATHReginaPutriAprizaBelum ada peringkat
- Papiloma PayudaraDokumen17 halamanPapiloma PayudaraDavid Restu Prasetia ManikBelum ada peringkat
- LAPORAN KASUS Kejang Demam Dhea.2-2Dokumen48 halamanLAPORAN KASUS Kejang Demam Dhea.2-2Herry GunawanBelum ada peringkat
- LBM 3 MataDokumen17 halamanLBM 3 MataShabryna ChouBelum ada peringkat
- Pertanyaan HerniaDokumen1 halamanPertanyaan HernianurhadiBelum ada peringkat
- Notulensi Tutorial Pertemuan 1 (Kelompok G - Modul 1)Dokumen10 halamanNotulensi Tutorial Pertemuan 1 (Kelompok G - Modul 1)Wah PutBelum ada peringkat
- Refleksi Kasus Od Subkonjungtival Bleeding Ec Trauma TumpulDokumen35 halamanRefleksi Kasus Od Subkonjungtival Bleeding Ec Trauma TumpulDrosophila Meilani GasterBelum ada peringkat
- SMKDokumen14 halamanSMKIrma AuliaBelum ada peringkat
- Lapsus MATA FixDokumen16 halamanLapsus MATA FixBagus SuryaBelum ada peringkat
- LP Sdry Eye SindromDokumen10 halamanLP Sdry Eye SindromAnonymous Hy8Tt602Belum ada peringkat
- Jejaring Diagram SHK Bayi Baru LahirDokumen1 halamanJejaring Diagram SHK Bayi Baru LahirhaninamaulianiBelum ada peringkat
- DT Sop UsgDokumen2 halamanDT Sop UsghaninamaulianiBelum ada peringkat
- DKK-PKM Orientasi Interop Alat USG Ke SI PKM Dan SatsetDokumen3 halamanDKK-PKM Orientasi Interop Alat USG Ke SI PKM Dan SatsethaninamaulianiBelum ada peringkat
- Surat Pemanggilan Peserta TKHKDokumen13 halamanSurat Pemanggilan Peserta TKHKhaninamaulianiBelum ada peringkat
- DATA Dan MATERI NEURODokumen7 halamanDATA Dan MATERI NEUROhaninamaulianiBelum ada peringkat
- Kebijakan Kesehatan Haji 2024Dokumen34 halamanKebijakan Kesehatan Haji 2024haninamaulianiBelum ada peringkat
- Form SURAT PENDELEGASIAN WEWENANGDokumen1 halamanForm SURAT PENDELEGASIAN WEWENANGhaninamaulianiBelum ada peringkat
- Evaluasi Pelaksanaan Binwin KUA Dari Aspek Kesehatan (Autosaved) (Autosaved)Dokumen20 halamanEvaluasi Pelaksanaan Binwin KUA Dari Aspek Kesehatan (Autosaved) (Autosaved)haninamaulianiBelum ada peringkat
- Soal 1Dokumen13 halamanSoal 1haninamaulianiBelum ada peringkat
- TES PAKET SOAL SINONIM DAN ANTONIMDokumen85 halamanTES PAKET SOAL SINONIM DAN ANTONIMSarasaBelum ada peringkat
- Laporan UKS DESEMBER 2021Dokumen26 halamanLaporan UKS DESEMBER 2021haninamaulianiBelum ada peringkat
- SE Akun Belajar - Id Sebagai SSO SIMPKBDokumen1 halamanSE Akun Belajar - Id Sebagai SSO SIMPKBYan WidhiBelum ada peringkat
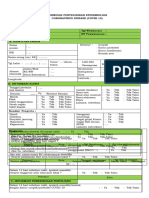
- Form PE CovidDokumen3 halamanForm PE CovidhaninamaulianiBelum ada peringkat
- Form Cuti Keperawatan Dan Penunjang MedisDokumen1 halamanForm Cuti Keperawatan Dan Penunjang Medissempak_pitungBelum ada peringkat
- Lembar Balik Kesehatan Reproduksi Dan Seksial Bagi Calon Pengantin PDFDokumen84 halamanLembar Balik Kesehatan Reproduksi Dan Seksial Bagi Calon Pengantin PDFchipa100% (3)
- Pemeriksaan Kesehatan Pra NikahDokumen34 halamanPemeriksaan Kesehatan Pra NikahhaninamaulianiBelum ada peringkat
- Form PE CovidDokumen3 halamanForm PE CovidhaninamaulianiBelum ada peringkat
- MQ. Salsabila-QS. Asy-Syams 2 & Al-Layl 1-13-02-22Dokumen19 halamanMQ. Salsabila-QS. Asy-Syams 2 & Al-Layl 1-13-02-22haninamaulianiBelum ada peringkat
- Sosialisasi Gerakan Pblhs Dinas PendidikanDokumen42 halamanSosialisasi Gerakan Pblhs Dinas PendidikanhaninamaulianiBelum ada peringkat
- Rencana Tindak LanjutDokumen3 halamanRencana Tindak LanjuthaninamaulianiBelum ada peringkat
- Penyakit Hati, Celah Dan Gangguan SetanDokumen8 halamanPenyakit Hati, Celah Dan Gangguan SetanhaninamaulianiBelum ada peringkat
- MQ. Salsabila QS. Asy Syams 06-02-22Dokumen14 halamanMQ. Salsabila QS. Asy Syams 06-02-22haninamaulianiBelum ada peringkat
- KemendikbudristekDokumen20 halamanKemendikbudristekChandra JuliantraBelum ada peringkat
- PEDOMAN PENGELOLAANDokumen44 halamanPEDOMAN PENGELOLAANDev DaraBelum ada peringkat
- SE Akun Belajar - Id Sebagai SSO SIMPKBDokumen1 halamanSE Akun Belajar - Id Sebagai SSO SIMPKBYan WidhiBelum ada peringkat
- RPK NewDokumen16 halamanRPK NewhaninamaulianiBelum ada peringkat
- MQ. Salsabila QS. Asy Syams 06-02-22Dokumen14 halamanMQ. Salsabila QS. Asy Syams 06-02-22haninamaulianiBelum ada peringkat
- Dokumen - Tips Partikel Materiatom Ion MolekulpptDokumen13 halamanDokumen - Tips Partikel Materiatom Ion MolekulpptDian Eka WijayaBelum ada peringkat
- Dzikir Dan Doa Mohon Perlindungan DiriDokumen3 halamanDzikir Dan Doa Mohon Perlindungan DirihaninamaulianiBelum ada peringkat
- RID COVID-19 v2Dokumen26 halamanRID COVID-19 v2haninamaulianiBelum ada peringkat