Anda mungkin juga menyukai
- Sosialisasi Penanganan DowntimeDokumen24 halamanSosialisasi Penanganan DowntimeMas'ud SubchiBelum ada peringkat
- HPK 2.5 Manajemen NyeriDokumen58 halamanHPK 2.5 Manajemen Nyeridede miswa septianiBelum ada peringkat
- Buku SingkatanDokumen48 halamanBuku Singkatanayu radianiBelum ada peringkat
- Dokumen Snars Edisi 1 Bab APDokumen26 halamanDokumen Snars Edisi 1 Bab APnanirakala100% (1)
- Laporan Kepatuhan Pemakaian Standar Kode Diagnosis Kode Tindakan Simbol Dan Singkatan 1 PDFDokumen15 halamanLaporan Kepatuhan Pemakaian Standar Kode Diagnosis Kode Tindakan Simbol Dan Singkatan 1 PDFbambang SutrionoBelum ada peringkat
- Surat Persetujuan Atau Penolakan Obat MahalDokumen1 halamanSurat Persetujuan Atau Penolakan Obat MahalUMIBelum ada peringkat
- Formulir Identifikasi NilaiDokumen1 halamanFormulir Identifikasi NilaiSemuel PanggaloBelum ada peringkat
- Form Rawat Jalan ProviderDokumen1 halamanForm Rawat Jalan ProviderDokternet Indonesia50% (2)
- Form KiupDokumen2 halamanForm KiupenikBelum ada peringkat
- AdMedika Authorization LetterDokumen2 halamanAdMedika Authorization LetterRS Kamar Medika AsuransiBelum ada peringkat
- Informed Consent VCT Klinik ResikDokumen2 halamanInformed Consent VCT Klinik ResikRSUD Serpong UtaraBelum ada peringkat
- 12.4 Terapi WicaraDokumen6 halaman12.4 Terapi WicaraNasrulM.YunusThaibBelum ada peringkat
- Spo Pengamanan Dan Kerahasian Rekam MedisDokumen2 halamanSpo Pengamanan Dan Kerahasian Rekam MedisSinta AyumiBelum ada peringkat
- SPO Pemberian Informasi Rekam MedisDokumen2 halamanSPO Pemberian Informasi Rekam MedisHevi YufriatnaBelum ada peringkat
- Pedoman Pengorganisasian RMDokumen66 halamanPedoman Pengorganisasian RMtri wardhanaBelum ada peringkat
- PANDUAN Penggunaan Daftar Singkatan, SImbol Dan Penulisan DiagnosisDokumen7 halamanPANDUAN Penggunaan Daftar Singkatan, SImbol Dan Penulisan DiagnosisarthurBelum ada peringkat
- Form Klaim AskridaDokumen1 halamanForm Klaim AskridaHidayah Nurul Hasanah Zen100% (1)
- OrientasiDokumen8 halamanOrientasiFitriana NurlaelaBelum ada peringkat
- RM. OK. 05 2019 - Catatan AnestesiDokumen2 halamanRM. OK. 05 2019 - Catatan AnestesiOom KomariahBelum ada peringkat
- Keterangan Cacat Tetap Akibat KecelakaanDokumen1 halamanKeterangan Cacat Tetap Akibat Kecelakaaneka candraBelum ada peringkat
- Formulir Klaim Rawat Inap Dan Pembedahan 2Dokumen2 halamanFormulir Klaim Rawat Inap Dan Pembedahan 2Elisa Gz100% (1)
- 3.2.2.1 Sop Penulisan Rekam Medis ElektronikDokumen3 halaman3.2.2.1 Sop Penulisan Rekam Medis Elektronikarie.ranuBelum ada peringkat
- Sensus Harian Rekam MedisDokumen6 halamanSensus Harian Rekam MedisMuslimEfendi100% (1)
- Pedoman Penyelenggaraan Mirm 2019Dokumen71 halamanPedoman Penyelenggaraan Mirm 2019Nurrahmi GhammamahBelum ada peringkat
- 6 Laporan Indeks Dokter Pasien Rawat Jalan April 2022Dokumen22 halaman6 Laporan Indeks Dokter Pasien Rawat Jalan April 2022rizkyBelum ada peringkat
- 7.1.1.1 Sop Pengisian Form Pendaftaran PasienDokumen2 halaman7.1.1.1 Sop Pengisian Form Pendaftaran PasienSiti Usmiranti UsmanBelum ada peringkat
- Alur Pelayanan Pasien Asuransi Rawat Jalan Inap GeneraliDokumen2 halamanAlur Pelayanan Pasien Asuransi Rawat Jalan Inap GeneraliYudhi setiawanBelum ada peringkat
- Daftar Formulir Rekam MedisDokumen2 halamanDaftar Formulir Rekam Medisyami indriyaniBelum ada peringkat
- Edukasi PasienDokumen2 halamanEdukasi Pasienklinik rahmatan lil alaminBelum ada peringkat
- Formulir Pendaftaran Pasien BaruDokumen1 halamanFormulir Pendaftaran Pasien Barunining fitrianyBelum ada peringkat
- Spo - Komunikasi - Efektif - Antar - Ppa - Dengan - Metode - Sbar - Dan - Read - BackDokumen2 halamanSpo - Komunikasi - Efektif - Antar - Ppa - Dengan - Metode - Sbar - Dan - Read - Backraka viarendraBelum ada peringkat
- Ringkasan Riwayat PoliklinikDokumen4 halamanRingkasan Riwayat PoliklinikYhayan EzVaro Vo'vizer100% (1)
- Draft Juknis Formulir Rekam Medis Rsud KotaDokumen36 halamanDraft Juknis Formulir Rekam Medis Rsud KotaWenny IrmawatiBelum ada peringkat
- Monev Kepatuhan FIXDokumen6 halamanMonev Kepatuhan FIXenik rohmaBelum ada peringkat
- Dokumen Pendukung TelemedicineDokumen11 halamanDokumen Pendukung Telemedicineprimades atriyantoBelum ada peringkat
- Asesmen Awal Pasien Rawat Inap: Hermina CiputatDokumen8 halamanAsesmen Awal Pasien Rawat Inap: Hermina CiputatInggrit KipuwBelum ada peringkat
- Persiapan Sebelum PitstopDokumen4 halamanPersiapan Sebelum Pitstopoctavia tri wulandariBelum ada peringkat
- Susunan Form RMDokumen26 halamanSusunan Form RMdillaBelum ada peringkat
- SK Pelaporan SirsDokumen1 halamanSK Pelaporan Sirssyivya123456678Belum ada peringkat
- 1 - Prosedur Pendaftaran Pasien Rawat JalanDokumen2 halaman1 - Prosedur Pendaftaran Pasien Rawat JalansumaryatiBelum ada peringkat
- Sop Pemakaian Nomor Rekam Medis Rangkap Di Tempat Penerimaan Dan Pendaftaran Pasien (TPP)Dokumen1 halamanSop Pemakaian Nomor Rekam Medis Rangkap Di Tempat Penerimaan Dan Pendaftaran Pasien (TPP)ulumBelum ada peringkat
- Daftar Kelengkapan Formulir RM RiDokumen2 halamanDaftar Kelengkapan Formulir RM RiDian FauziahBelum ada peringkat
- Evaluasi SIKDA OptimaDokumen25 halamanEvaluasi SIKDA Optimajannah_30Belum ada peringkat
- Formula Pada Ms. ExcelDokumen11 halamanFormula Pada Ms. ExcelSari AnnaBelum ada peringkat
- Form Klaim Rawat JalanDokumen1 halamanForm Klaim Rawat JalanDanHasanBelum ada peringkat
- Spo Penerimaan Pasien Dengan Jaminan Pelayanan KesehatanDokumen2 halamanSpo Penerimaan Pasien Dengan Jaminan Pelayanan KesehatanMadrid PoohBelum ada peringkat
- Persetujuan Rawat Inap Dan Penolakan Rawat Inap PDFDokumen2 halamanPersetujuan Rawat Inap Dan Penolakan Rawat Inap PDFIka NovelitaBelum ada peringkat
- 7 Juklak Pengisian FORM RMDokumen28 halaman7 Juklak Pengisian FORM RMNiniez IndrawatiBelum ada peringkat
- 3.8.1 Ep 1 Spo Pengembalian Rekam MedisDokumen2 halaman3.8.1 Ep 1 Spo Pengembalian Rekam Medispuskesmas panyileukanBelum ada peringkat
- BPPRM (Buku Pedoman Penyelenggaraan Rekam Medis) Tahun 2022Dokumen185 halamanBPPRM (Buku Pedoman Penyelenggaraan Rekam Medis) Tahun 2022indamshBelum ada peringkat
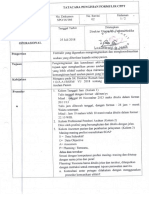
- SPO Tatacara Pengisian CPPTDokumen2 halamanSPO Tatacara Pengisian CPPTJoni Numiarto LBelum ada peringkat
- Buku Pedoman Survei KARS - Edit 16 Agustus 2012Dokumen35 halamanBuku Pedoman Survei KARS - Edit 16 Agustus 2012Safiqulatif Abdillah100% (2)
- Spo Informasi Informed ConsentDokumen2 halamanSpo Informasi Informed ConsentdrgdikaBelum ada peringkat
- Form RJ & Dental MedilinkDokumen1 halamanForm RJ & Dental Medilinkrsjmc rajal123Belum ada peringkat
- Form Verifikasi InacbgDokumen1 halamanForm Verifikasi InacbgAndrew SatryaBelum ada peringkat
- SOP Penyimpanan Dokumen Rekam MedisDokumen2 halamanSOP Penyimpanan Dokumen Rekam MedisAnonymous 67855CnL100% (1)
- Spo Rawat JalanDokumen3 halamanSpo Rawat JalanajudBelum ada peringkat
- Sistem Registrasi Kanker Di Indonesia SrikandiDokumen32 halamanSistem Registrasi Kanker Di Indonesia SrikandiSuanjayaagusBelum ada peringkat
- Surat Keterangan Dokter (Physician Form) Rawat Inap/HospitalizationDokumen2 halamanSurat Keterangan Dokter (Physician Form) Rawat Inap/HospitalizationjohnnyBelum ada peringkat
- Surat Keterangan Dokter HospitalizationDokumen2 halamanSurat Keterangan Dokter HospitalizationAdi Puspani JhaBelum ada peringkat
- Laporan Sosialisasi SKP - 2Dokumen4 halamanLaporan Sosialisasi SKP - 2hardinoBelum ada peringkat
- Doa Upacara SeninDokumen7 halamanDoa Upacara SeninhardinoBelum ada peringkat
- Standar Pelayanan Terapi OkupasiDokumen11 halamanStandar Pelayanan Terapi OkupasihardinoBelum ada peringkat
- Laporan Sosialisasi SKP - 1Dokumen2 halamanLaporan Sosialisasi SKP - 1hardinoBelum ada peringkat
- Form Kuning MESODokumen2 halamanForm Kuning MESOurtical100% (2)
- Form Checklist Review Obat PasienDokumen4 halamanForm Checklist Review Obat PasienhardinoBelum ada peringkat
- Pengiriman Spesimen Dahak Untuk Pemeriksan Tcm1Dokumen2 halamanPengiriman Spesimen Dahak Untuk Pemeriksan Tcm1hardinoBelum ada peringkat
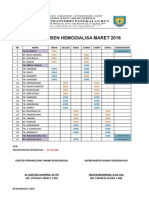
- Laporan Bulanan HDDokumen37 halamanLaporan Bulanan HDhardinoBelum ada peringkat
- Tes Cepat Molekuler (TCM)Dokumen18 halamanTes Cepat Molekuler (TCM)hardino100% (2)
- Doa Upacara Senin PDFDokumen1 halamanDoa Upacara Senin PDFhardinoBelum ada peringkat
- Etika Aparatur Dalam Pelayanan PublikDokumen25 halamanEtika Aparatur Dalam Pelayanan Publikhardino0% (1)
- Pedoman Organisasi HDDokumen21 halamanPedoman Organisasi HDhardino100% (3)
- Rencana Perubahan 2018Dokumen26 halamanRencana Perubahan 2018hardinoBelum ada peringkat
- Doa Upacara Senin PDFDokumen1 halamanDoa Upacara Senin PDFhardinoBelum ada peringkat