Anda mungkin juga menyukai
- Coronavirus Covid-19. Membela diri. Cara menghindari penularan. Bagaimana melindungi keluarga dan pekerjaan Anda. Diperbarui edisi keempat.Dari EverandCoronavirus Covid-19. Membela diri. Cara menghindari penularan. Bagaimana melindungi keluarga dan pekerjaan Anda. Diperbarui edisi keempat.Penilaian: 5 dari 5 bintang5/5 (2)
- PPOK STABIL Dan EKSASERBASIDokumen51 halamanPPOK STABIL Dan EKSASERBASIAlma SyavhanieBelum ada peringkat
- PPOK - DR MasrulDokumen45 halamanPPOK - DR MasrulgitafazaBelum ada peringkat
- Kenali Dan Deteksi Dini PPOKDokumen56 halamanKenali Dan Deteksi Dini PPOKReyvanly Hizkia ThiosBelum ada peringkat
- Penyakit Paru Obstruktif KronikDokumen38 halamanPenyakit Paru Obstruktif KronikYudistra R ShafarlyBelum ada peringkat
- PPOKDokumen60 halamanPPOKHolly RiyadiBelum ada peringkat
- Ppok Stabil Dan Eksersebasi Fix Adilla EditDokumen54 halamanPpok Stabil Dan Eksersebasi Fix Adilla EditAdhyllatata EvandBelum ada peringkat
- PPOKDokumen60 halamanPPOKKhoirotun NisaBelum ada peringkat
- CHF PpokDokumen57 halamanCHF PpokAfifah Haifa PutriBelum ada peringkat
- Penyakit Paru Obsbtruktif KronikDokumen18 halamanPenyakit Paru Obsbtruktif KronikDiah AndiniBelum ada peringkat
- PPOKDokumen10 halamanPPOKputu ayu masrianiBelum ada peringkat
- PpokDokumen103 halamanPpokSukmawati Eka Bima SahputriBelum ada peringkat
- Crs PpokDokumen28 halamanCrs PpokfairuzfauziaBelum ada peringkat
- Skripsi Risa PpokDokumen48 halamanSkripsi Risa Ppokyogha100% (1)
- Tatalaksana PpokDokumen39 halamanTatalaksana Ppokdokter1991Belum ada peringkat
- Copd ManagementDokumen31 halamanCopd ManagementRosi AmaliaBelum ada peringkat
- Surveilans PPOKDokumen33 halamanSurveilans PPOKErvina NoviantiBelum ada peringkat
- Skrining PPOK Pandu PTM - 19Dec2023-PDPIDokumen40 halamanSkrining PPOK Pandu PTM - 19Dec2023-PDPILaeli Nur MaeniBelum ada peringkat
- Riview PPOK CandraDokumen32 halamanRiview PPOK CandraSri WahyuniBelum ada peringkat
- PPOK UpdateDokumen40 halamanPPOK UpdatePandaBelum ada peringkat
- Referat PPOKDokumen36 halamanReferat PPOKaditiarrtuguBelum ada peringkat
- Css-Gina Gold 2223 NandaDokumen52 halamanCss-Gina Gold 2223 NandaNanda FLBelum ada peringkat
- Makalah PPOK ParuDokumen19 halamanMakalah PPOK ParuSatriani JeeBelum ada peringkat
- 3.3 Tatalaksana PPOK Deva Jrcu 20ok19Dokumen37 halaman3.3 Tatalaksana PPOK Deva Jrcu 20ok19alyaBelum ada peringkat
- Ppok WordDokumen13 halamanPpok Wordzainal arifinBelum ada peringkat
- Jurnal PPOKDokumen16 halamanJurnal PPOKMuhammad Kahfi100% (2)
- Laporan Pendahuluan PpokDokumen16 halamanLaporan Pendahuluan PpokVena RitemBelum ada peringkat
- Referat COPD EditedDokumen15 halamanReferat COPD EditedElizabeth Joan SalimBelum ada peringkat
- Case PPOKDokumen33 halamanCase PPOKYoana FebriBelum ada peringkat
- CSS - PpokDokumen21 halamanCSS - PpokayuniputriBelum ada peringkat
- 56hsu JdjsunjjjDokumen14 halaman56hsu JdjsunjjjRoyyan 27Belum ada peringkat
- LP PPOK Zaitun 1 FiksDokumen12 halamanLP PPOK Zaitun 1 FiksJarry-OfficielBelum ada peringkat
- PPOK Afandi Setia Apriliyan FETP 2306305105Dokumen43 halamanPPOK Afandi Setia Apriliyan FETP 2306305105ferdiiqoBelum ada peringkat
- Referat PPOK Widya Ayu Putri Maharani - 182011101004 - FIXDokumen70 halamanReferat PPOK Widya Ayu Putri Maharani - 182011101004 - FIXdila2706Belum ada peringkat
- Buku Saku PPOKDokumen55 halamanBuku Saku PPOKFajar ApriliyansahBelum ada peringkat
- Ppok DG TX KortikoDokumen26 halamanPpok DG TX KortikolindaBelum ada peringkat
- Skenario 2Dokumen16 halamanSkenario 22020A05Muhammad Nadhil MaulidyBelum ada peringkat
- Case PPOKDokumen32 halamanCase PPOKSigusBelum ada peringkat
- PPOK Nomensen 2019Dokumen28 halamanPPOK Nomensen 2019MICHABelum ada peringkat
- Referat PPOKDokumen27 halamanReferat PPOKAmirah PuspitaBelum ada peringkat
- Makalah Farmakoterapi Ii PpokDokumen16 halamanMakalah Farmakoterapi Ii PpokAyhu Risky GamoroBelum ada peringkat
- Penyakit Paru Obstruktif KronikDokumen7 halamanPenyakit Paru Obstruktif KronikArnisa AmaliaBelum ada peringkat
- PPOKDokumen31 halamanPPOKAisyatu Al FinaBelum ada peringkat
- Makalah PPOKDokumen10 halamanMakalah PPOKrisa tifaBelum ada peringkat
- Bahan Ppok EditDokumen45 halamanBahan Ppok Editriri permata sariBelum ada peringkat
- Acute Exacerbation of CopdDokumen37 halamanAcute Exacerbation of CopdCah BagoesBelum ada peringkat
- Refarat Related MustajirDokumen26 halamanRefarat Related MustajirIrma SihotangBelum ada peringkat
- Case Report PPOK - Stase Paru - Melvy RozaDokumen61 halamanCase Report PPOK - Stase Paru - Melvy RozaMelvy RozaBelum ada peringkat
- Referat Ppok-Rokok RRDokumen25 halamanReferat Ppok-Rokok RRLalu Reza AldiraBelum ada peringkat
- Ppok Baru Gold 2018Dokumen53 halamanPpok Baru Gold 2018AbrorMuhammad100% (1)
- Penyakit Paru Obstruktif KronikDokumen22 halamanPenyakit Paru Obstruktif Kronikd intan pBelum ada peringkat
- Bab IiDokumen21 halamanBab IiNUR ICHLAS ROFA PUTRABelum ada peringkat
- BAB I BismillahDokumen31 halamanBAB I BismillahArafah RubyBelum ada peringkat
- Lnjut Dsni 2Dokumen54 halamanLnjut Dsni 2Paramita MusaBelum ada peringkat
- Makalah PpokDokumen19 halamanMakalah PpokRocky MawaraBelum ada peringkat
- Mikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaDari EverandMikrobiologi Perubatan I: Patogen dan Mikrobiologi ManusiaPenilaian: 2.5 dari 5 bintang2.5/5 (2)
- Mikrobiologi Medis I: Patogen dan Mikrobioma ManusiaDari EverandMikrobiologi Medis I: Patogen dan Mikrobioma ManusiaPenilaian: 4 dari 5 bintang4/5 (11)
- H2 Topik 4.1 - DR Yeni Hidrokortison FixDokumen25 halamanH2 Topik 4.1 - DR Yeni Hidrokortison FixRosi AmaliaBelum ada peringkat
- H2 Topik 4.2 - Dr. Deddy Antileukotrien Revisi 2Dokumen24 halamanH2 Topik 4.2 - Dr. Deddy Antileukotrien Revisi 2Rosi AmaliaBelum ada peringkat
- Tatalaksana TBDokumen49 halamanTatalaksana TBRosi AmaliaBelum ada peringkat
- H2 Topik 3.1 - Dr. Oea - Role of Oxygen TherapyDokumen32 halamanH2 Topik 3.1 - Dr. Oea - Role of Oxygen TherapyRosi AmaliaBelum ada peringkat
- H2 Topik 5.2 - Dr. Oea Update EPG (1) - OKDokumen23 halamanH2 Topik 5.2 - Dr. Oea Update EPG (1) - OKRosi AmaliaBelum ada peringkat
- Copd ManagementDokumen31 halamanCopd ManagementRosi AmaliaBelum ada peringkat
- TB SoDokumen48 halamanTB SoRosi AmaliaBelum ada peringkat
- Simple ApproachDokumen36 halamanSimple ApproachRosi AmaliaBelum ada peringkat
- Covid Update ManagementDokumen26 halamanCovid Update ManagementRosi AmaliaBelum ada peringkat
- Peran Nutrisi DG HMB & Triple Protein Pada PPOKDokumen30 halamanPeran Nutrisi DG HMB & Triple Protein Pada PPOKRosi AmaliaBelum ada peringkat
- Covid 19Dokumen28 halamanCovid 19Rosi AmaliaBelum ada peringkat
- BronchosDokumen36 halamanBronchosRosi AmaliaBelum ada peringkat
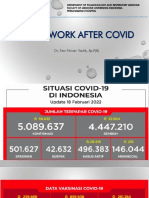
- Fit To Work After CovidDokumen27 halamanFit To Work After CovidRosi AmaliaBelum ada peringkat
- TB Laten2Dokumen25 halamanTB Laten2Rosi AmaliaBelum ada peringkat
- Ppi Covid Idi 2Dokumen1 halamanPpi Covid Idi 2Rosi AmaliaBelum ada peringkat
- Peran Vit D3 Pada Penangan Long CovidDokumen28 halamanPeran Vit D3 Pada Penangan Long CovidRosi AmaliaBelum ada peringkat
- Genomic Dan Non GenomicDokumen34 halamanGenomic Dan Non GenomicRosi AmaliaBelum ada peringkat
- Ppok Batam 2022Dokumen74 halamanPpok Batam 2022Rosi AmaliaBelum ada peringkat
- Dosis Dopamin DobutaminDokumen4 halamanDosis Dopamin DobutaminRosi AmaliaBelum ada peringkat
- Tatalaksana HYPOXEMIADokumen28 halamanTatalaksana HYPOXEMIARosi AmaliaBelum ada peringkat
- 10.10-10.35 Dr. Widya Sri Hastuti SP.P Asma Eksaserbasi Pdpi KepriDokumen30 halaman10.10-10.35 Dr. Widya Sri Hastuti SP.P Asma Eksaserbasi Pdpi KepriRosi AmaliaBelum ada peringkat
- Buku Pedoman Tatalaksana COVID-19 5OP Edisi 3 2020Dokumen149 halamanBuku Pedoman Tatalaksana COVID-19 5OP Edisi 3 2020iard6447Belum ada peringkat
- Ppi Covid Idi 2Dokumen1 halamanPpi Covid Idi 2Rosi AmaliaBelum ada peringkat
- KMK No. HK.01.07 MENKES 707 2018 Perubahan Fornas 1Dokumen73 halamanKMK No. HK.01.07 MENKES 707 2018 Perubahan Fornas 1Dogol Suryonugroho100% (2)
- BAB I HepatitisDokumen1 halamanBAB I HepatitisRosi AmaliaBelum ada peringkat
- Referat KolesteatomaDokumen17 halamanReferat KolesteatomaRosi AmaliaBelum ada peringkat
- Dosis Dopamin DobutaminDokumen4 halamanDosis Dopamin DobutaminRosi AmaliaBelum ada peringkat
- Buku Dosis Obat Anak IdaipdfDokumen160 halamanBuku Dosis Obat Anak IdaipdfRosi AmaliaBelum ada peringkat
- Referat Trauma Tumpul OculliDokumen12 halamanReferat Trauma Tumpul OculliRosi AmaliaBelum ada peringkat