Anda mungkin juga menyukai
- Tugas Skdi Kelompok Coass Xi CDokumen218 halamanTugas Skdi Kelompok Coass Xi CTedi MulyanaBelum ada peringkat
- Fisiologi Sistem Saraf Dasar - StudentsDokumen45 halamanFisiologi Sistem Saraf Dasar - StudentsAndi Dachri0% (1)
- Pankreatit IsDokumen71 halamanPankreatit IsIkha MarahkiyahBelum ada peringkat
- Obat Anestesi Lokal 97Dokumen23 halamanObat Anestesi Lokal 97FP_wardhaBelum ada peringkat
- EPISTAKSISDokumen24 halamanEPISTAKSISSulistyaning TyasBelum ada peringkat
- Metabolisme OtakDokumen33 halamanMetabolisme Otakikhy100% (1)
- Laporan Kasus B20 Dengan Komplikasi Chepalgia DR - Nurhidayat.Dokumen11 halamanLaporan Kasus B20 Dengan Komplikasi Chepalgia DR - Nurhidayat.Aldino Siwa PutraBelum ada peringkat
- GoiterDokumen6 halamanGoiterPitaloka YuniartiningtyasBelum ada peringkat
- Modul KesemutanDokumen64 halamanModul KesemutanAriefBelum ada peringkat
- NEUROPATI DAN MIOPATIDokumen29 halamanNEUROPATI DAN MIOPATIAbdur Rahman100% (1)
- KatarakDokumen65 halamanKatarakFarah AkhwanisBelum ada peringkat
- Sop Ismki Action EditDokumen6 halamanSop Ismki Action EditMutiahf98100% (1)
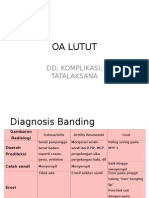
- OA LUTUT DD Komplikasi TatalaksanaDokumen8 halamanOA LUTUT DD Komplikasi TatalaksanaNatisha DivyaBelum ada peringkat
- Step 7: Anatomi HidungDokumen28 halamanStep 7: Anatomi HidungAnonymous J8AyRTBelum ada peringkat
- MENGOBATI MATA MERAHDokumen9 halamanMENGOBATI MATA MERAHAnonymous hxXpvZdZBelum ada peringkat
- Rencana EvakuasiDokumen22 halamanRencana EvakuasiMuhamad ChomsulBelum ada peringkat
- ProposalDokumen17 halamanProposalnadhira.daniswaraBelum ada peringkat
- PapiledemaDokumen12 halamanPapiledemaignatiuserikBelum ada peringkat
- Makalah Special Sense SystemDokumen22 halamanMakalah Special Sense SystemMarisa Khairani HazrinaBelum ada peringkat
- Makalah Tear FilmDokumen18 halamanMakalah Tear FilmalpasraekaBelum ada peringkat
- ENTROPIONDokumen25 halamanENTROPIONAnthony ChandraBelum ada peringkat
- Jurnal Reading MalariaDokumen17 halamanJurnal Reading MalariadiyanahBelum ada peringkat
- PR Minggu 1Dokumen8 halamanPR Minggu 1firman madao234Belum ada peringkat
- Pemeriksaan Tanda Rangsang Meningeal Dan Tingkat KesadaranDokumen7 halamanPemeriksaan Tanda Rangsang Meningeal Dan Tingkat KesadaranNovia Dwi TirtasariBelum ada peringkat
- Kejang DemamDokumen72 halamanKejang Demamelita purnamaBelum ada peringkat
- Tatalaksana Sumbat HidungDokumen30 halamanTatalaksana Sumbat HidungauditiavicaBelum ada peringkat
- Sindroma EkstrapiramidalDokumen6 halamanSindroma EkstrapiramidalDisa NugrahaBelum ada peringkat
- Tatalaksana OtomikosisDokumen3 halamanTatalaksana OtomikosisfatinfatharaniBelum ada peringkat
- ANESTESI PADA IKTERUS OBSTRUKTIFDokumen71 halamanANESTESI PADA IKTERUS OBSTRUKTIFardiansyahBelum ada peringkat
- DELAYED UNIONDokumen8 halamanDELAYED UNIONulfi saputriBelum ada peringkat
- Kajian Urgensi MoratoriumDokumen19 halamanKajian Urgensi MoratoriumPutri BalqisBelum ada peringkat
- Modul KK SirkumsisiDokumen8 halamanModul KK SirkumsisiADELIA YUNIKA UTAMIBelum ada peringkat
- Referat Anestesi EpiduralDokumen20 halamanReferat Anestesi EpiduralYopi Anugrah WatiBelum ada peringkat
- Hemangioma Cavernous Juga Disebut SebagaiDokumen5 halamanHemangioma Cavernous Juga Disebut SebagaiAnnie BukangBelum ada peringkat
- DETEKSI DINI KANKER PAYUDARADokumen39 halamanDETEKSI DINI KANKER PAYUDARAMariaBelum ada peringkat
- Deskripsi Tertutup Reposisi TulangDokumen3 halamanDeskripsi Tertutup Reposisi TulangDianSelviaBelum ada peringkat
- DOKUMENDokumen13 halamanDOKUMENputriarum100% (1)
- Crs GastroschisisDokumen6 halamanCrs GastroschisisRosatya ImanuelaBelum ada peringkat
- KOMUNIKASI PESISIRDokumen17 halamanKOMUNIKASI PESISIRWidyawati SasmitaBelum ada peringkat
- Diagnosis Kejang Dan Movement DisorderDokumen43 halamanDiagnosis Kejang Dan Movement DisorderM.Ardaris AlhudriBelum ada peringkat
- (Status Ujian) Hemoroid EksternaDokumen11 halaman(Status Ujian) Hemoroid EksternaNuraga Dwi PratapaBelum ada peringkat
- HistologiMataDokumen4 halamanHistologiMataKrisliana JeaneBelum ada peringkat
- Phantom MataDokumen9 halamanPhantom MataJel JelitaaaBelum ada peringkat
- Sistem Saraf OtonomDokumen32 halamanSistem Saraf OtonomkadiksuhBelum ada peringkat
- Obat Antagonis OpioidDokumen10 halamanObat Antagonis OpioidTarsisius Ryang TobyBelum ada peringkat
- RESEP MATADokumen28 halamanRESEP MATAlailatut toriqohBelum ada peringkat
- Agia Katarak KomplikataDokumen19 halamanAgia Katarak KomplikataAgia_Omink_Nug_5666Belum ada peringkat
- PPK Uveitis Anterior AkutDokumen5 halamanPPK Uveitis Anterior AkutKlinik Mata EDC TulungagungBelum ada peringkat
- Tatalaksana Anemia Pada Gagal Ginjal KronikDokumen25 halamanTatalaksana Anemia Pada Gagal Ginjal KronikNurlaili Yani100% (2)
- MataDokumen14 halamanMatafinaBelum ada peringkat
- GANGGUAN PERKEMBANGANDokumen48 halamanGANGGUAN PERKEMBANGANHendra ErchaririBelum ada peringkat
- Anatomi Histologi EmpeduDokumen5 halamanAnatomi Histologi EmpeduyogidjBelum ada peringkat
- Keratitis pada Perempuan 35 TahunDokumen12 halamanKeratitis pada Perempuan 35 TahunKoko ImronBelum ada peringkat
- Anatomi Dan Fisiologi UveaDokumen15 halamanAnatomi Dan Fisiologi UveaAlmira WilonnaBelum ada peringkat
- KOMPLIKASI FRAKTURDokumen4 halamanKOMPLIKASI FRAKTURArya Putra SyuhadaBelum ada peringkat
- Pemeriksaan Mata, Dr. SuliatiDokumen52 halamanPemeriksaan Mata, Dr. SuliatiIndri Meliawati RadisuBelum ada peringkat
- Bab II Polip SinonasalDokumen19 halamanBab II Polip SinonasalBobby S PromondoBelum ada peringkat
- BST Atresia AniDokumen29 halamanBST Atresia Ani----Belum ada peringkat
- Presentation Fix UlkusDokumen20 halamanPresentation Fix UlkusginanjarBelum ada peringkat
- Kelainan KorneaDokumen50 halamanKelainan KorneaKhaidirBelum ada peringkat
- Kelalaian MedikDokumen37 halamanKelalaian MedikVissalini JayabalanBelum ada peringkat
- HAM RUANG LINGKUPDokumen4 halamanHAM RUANG LINGKUPVissalini JayabalanBelum ada peringkat
- Penulisan Laporan Penelitian1Dokumen29 halamanPenulisan Laporan Penelitian1Vissalini JayabalanBelum ada peringkat
- HAM-KesehatanDokumen30 halamanHAM-KesehatanEva Marini SimbolonBelum ada peringkat
- Ketahanan NasionalDokumen20 halamanKetahanan NasionalVissalini JayabalanBelum ada peringkat
- Anatomi Dan Fisiologi MataDokumen30 halamanAnatomi Dan Fisiologi MataDanti Nelfa RizaBelum ada peringkat
- BAB I AnastesiDokumen5 halamanBAB I AnastesiVissalini JayabalanBelum ada peringkat
- Chapter IIDokumen13 halamanChapter IIReynalth Andrew SinagaBelum ada peringkat
- K - 3 Determinan PerilakuDokumen15 halamanK - 3 Determinan PerilakuVissalini JayabalanBelum ada peringkat
- Visum Et Repertum Dan Prosedur Pemeriksaan Kedokteran ForensikDokumen16 halamanVisum Et Repertum Dan Prosedur Pemeriksaan Kedokteran ForensikVissalini JayabalanBelum ada peringkat
- EtiologiDokumen13 halamanEtiologiVissalini JayabalanBelum ada peringkat
- Hallmark of CancerDokumen27 halamanHallmark of CancerVissalini Jayabalan100% (2)
- Gambaran Nematoda Usus Pada Kecoa Dari Rumah Makan Dan Restoran Jalan DR Mansur Medan 2012 (Manuskript)Dokumen12 halamanGambaran Nematoda Usus Pada Kecoa Dari Rumah Makan Dan Restoran Jalan DR Mansur Medan 2012 (Manuskript)Vissalini Jayabalan0% (1)
- ReferenceDokumen3 halamanReferenceVissalini JayabalanBelum ada peringkat
- Anatomi Kelenjar EndoktrinDokumen3 halamanAnatomi Kelenjar EndoktrinNadia AviantyBelum ada peringkat
- Daftar PustakaDokumen1 halamanDaftar PustakaVissalini JayabalanBelum ada peringkat
- BAB 1 Kti CoassDokumen28 halamanBAB 1 Kti CoassVissalini JayabalanBelum ada peringkat
- MENGKAS ENDDokumen15 halamanMENGKAS ENDNitaRohmanita Adalah IedaMaryatiBelum ada peringkat
- KOMPLIKASIDokumen2 halamanKOMPLIKASIVissalini JayabalanBelum ada peringkat
- Makalah Pediatrik SosialDokumen1 halamanMakalah Pediatrik SosialVissalini JayabalanBelum ada peringkat
- Makalah Forensik CoverDokumen1 halamanMakalah Forensik CoverParvinaa VnaBelum ada peringkat
- 14 PsikosisDokumen20 halaman14 PsikosisIrham TahkikBelum ada peringkat
- Laporan KasusDokumen2 halamanLaporan KasusVissalini JayabalanBelum ada peringkat
- Klasifikasi Tumor Sellar Dan ParasellarDokumen25 halamanKlasifikasi Tumor Sellar Dan ParasellarVissalini JayabalanBelum ada peringkat
- Otitis Media Supuratif KronikDokumen30 halamanOtitis Media Supuratif Kronikhidyia100% (1)
- Bayi Dengan Hipotiroidisme KonginitalDokumen16 halamanBayi Dengan Hipotiroidisme KonginitalVissalini JayabalanBelum ada peringkat
- Powerpoint Neuro CompleteDokumen67 halamanPowerpoint Neuro CompleteVissalini Jayabalan100% (2)
- BAB 2 OmskDokumen23 halamanBAB 2 OmskVissalini JayabalanBelum ada peringkat
- Otitis Media Supuratif KronisDokumen34 halamanOtitis Media Supuratif KronisVissalini JayabalanBelum ada peringkat