Anda mungkin juga menyukai
- Case Report Neonatus InfeksiDokumen37 halamanCase Report Neonatus InfeksiErwin ImawanBelum ada peringkat
- DEMAM CHIKUNGUNYADokumen18 halamanDEMAM CHIKUNGUNYASarachanda SallyBelum ada peringkat
- PPH FAMILIALDokumen4 halamanPPH FAMILIALrahayuBelum ada peringkat
- SECTIO CAESAREADokumen41 halamanSECTIO CAESAREAraranaomi29Belum ada peringkat
- Journal Reading SepsisDokumen39 halamanJournal Reading SepsisbebyBelum ada peringkat
- CrsDokumen45 halamanCrsWinarti RimadhaniBelum ada peringkat
- EPIDEMI LEPTODokumen33 halamanEPIDEMI LEPTONina Barorotul Mutmainnah100% (1)
- Lapkas Anak Glomerulonefritis AkutDokumen32 halamanLapkas Anak Glomerulonefritis AkutPutri YowanaBelum ada peringkat
- Referat Hipertensi EmergensiDokumen4 halamanReferat Hipertensi EmergensiSicillia AgusBelum ada peringkat
- PERDARAHANDokumen31 halamanPERDARAHANokkiemsBelum ada peringkat
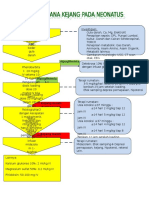
- Tatalaksana Kejang NeonatusDokumen1 halamanTatalaksana Kejang NeonatusMerlyn_RumtheBelum ada peringkat
- PGD NeonatusDokumen41 halamanPGD NeonatusZulfa N. FathBelum ada peringkat
- Crs BKCDokumen27 halamanCrs BKCrafersBelum ada peringkat
- CASE Bedah Dwi OktaviliaDokumen40 halamanCASE Bedah Dwi OktaviliaPurryBelum ada peringkat
- Antipiretik vs Antipiretik+SponsDokumen36 halamanAntipiretik vs Antipiretik+SponsCitraBelum ada peringkat
- Diagnosis Dan Tata Laksana DBD - Handout - 19jan2019 PDFDokumen48 halamanDiagnosis Dan Tata Laksana DBD - Handout - 19jan2019 PDFJhoeDjiplak100% (1)
- Case Report BPHDokumen28 halamanCase Report BPHanggun pratissaBelum ada peringkat
- DEMAM DENGUEDokumen41 halamanDEMAM DENGUEWulanbumuloBelum ada peringkat
- PRINSIP REHIDRASI PADA ANAK DENGAN DEHIDRASIDokumen40 halamanPRINSIP REHIDRASI PADA ANAK DENGAN DEHIDRASInouval_iqbalBelum ada peringkat
- Lefrat Nasofaringitis EchaDokumen15 halamanLefrat Nasofaringitis EchaEchaaBelum ada peringkat
- ISKDokumen18 halamanISKRudy KgBelum ada peringkat
- Partus Terlantar (Neglected Labour)Dokumen19 halamanPartus Terlantar (Neglected Labour)chaliddaulayBelum ada peringkat
- Fluid & Electrolyte Therapy MedsenseDokumen90 halamanFluid & Electrolyte Therapy Medsensefadilah rizky167Belum ada peringkat
- Edukasi Cara Menghitung Kebutuhan Kalori Pada Pasien Sindroma MetabolikDokumen10 halamanEdukasi Cara Menghitung Kebutuhan Kalori Pada Pasien Sindroma MetabolikAyu Mulya Lestari AviantoBelum ada peringkat
- GNAPSDokumen59 halamanGNAPSferinanatasyaBelum ada peringkat
- Demam TifoidDokumen29 halamanDemam TifoidPutri PermatasariBelum ada peringkat
- Laporan Kasus Polisitemia Vera FixDokumen11 halamanLaporan Kasus Polisitemia Vera FixIqyu Chan KyuBelum ada peringkat
- Diagnostik AmlDokumen27 halamanDiagnostik AmlemmiBelum ada peringkat
- INTERPRETASI HIPERFERITINEMIADokumen6 halamanINTERPRETASI HIPERFERITINEMIAJoan Vinata WinonaBelum ada peringkat
- Case Morbili Dengan Komplikasi BronkopneumoniaDokumen67 halamanCase Morbili Dengan Komplikasi BronkopneumoniaRudySyahputraDaulayBelum ada peringkat
- Tata Laksana Anak Pendek PDFDokumen50 halamanTata Laksana Anak Pendek PDFBayu KurniawanBelum ada peringkat
- Laporan Kasus - KolelitiasisDokumen42 halamanLaporan Kasus - Kolelitiasisherlin pyBelum ada peringkat
- MEGANITA (Perdarahan Trimester 1)Dokumen29 halamanMEGANITA (Perdarahan Trimester 1)dyahayulestariBelum ada peringkat
- Dr. H Syafruddin Arl, Sppd-Kgeh MarsDokumen37 halamanDr. H Syafruddin Arl, Sppd-Kgeh MarsarriesutantoBelum ada peringkat
- STATUS EPILEPTIKUSDokumen32 halamanSTATUS EPILEPTIKUSIntan AliBelum ada peringkat
- Dokumen tentang Duh Tubuh VaginaDokumen35 halamanDokumen tentang Duh Tubuh VaginaipdBelum ada peringkat
- ITPDokumen15 halamanITPJoviantoReynoldAndikaHidayatBelum ada peringkat
- TB Kutis - DR - DinaDokumen48 halamanTB Kutis - DR - DinaDimas Rifqy HabibieBelum ada peringkat
- Kelompok A.2Dokumen7 halamanKelompok A.2Agung IndraBelum ada peringkat
- Penangan Kad HHSDokumen10 halamanPenangan Kad HHSEvan ErnandiBelum ada peringkat
- Laporan Kasus Tinea PedisDokumen35 halamanLaporan Kasus Tinea PedisVega PaathBelum ada peringkat
- PPK MalariaDokumen4 halamanPPK MalariaFanny TimungBelum ada peringkat
- KetDokumen13 halamanKetLulu azzahraBelum ada peringkat
- Respirologi AnakDokumen92 halamanRespirologi AnakReza MuhammadBelum ada peringkat
- LAPORAN KASUS PJBDokumen63 halamanLAPORAN KASUS PJBAnonymous kdAN6T100% (1)
- HIPERTENSI DALAM KEHAMILANDokumen24 halamanHIPERTENSI DALAM KEHAMILANtessa wulandariBelum ada peringkat
- Hepatitis FulminanDokumen8 halamanHepatitis FulminanAntique HuntoyungoBelum ada peringkat
- Referat DMDokumen39 halamanReferat DMsiti hazard aldinaBelum ada peringkat
- Case AIHADokumen31 halamanCase AIHAMeiustia Rahayu, MDBelum ada peringkat
- REKOMENDASI Penatalaksanaan Kejang DemamDokumen25 halamanREKOMENDASI Penatalaksanaan Kejang DemamRohmah dini nur kusumaBelum ada peringkat
- OkeDokumen9 halamanOkekarnoBelum ada peringkat
- Mini Project "Intervensi Pada Pasien Penyakit Ispa Pada Anak " Puskesmas Salobulo, Kabupaten WajoDokumen38 halamanMini Project "Intervensi Pada Pasien Penyakit Ispa Pada Anak " Puskesmas Salobulo, Kabupaten WajoepingBelum ada peringkat
- KEHAMILANEKTOPIKDokumen36 halamanKEHAMILANEKTOPIKPinondangGabriellaTobingBelum ada peringkat
- Panduan Praktik Klinis DisentriDokumen3 halamanPanduan Praktik Klinis DisentriRahaswinBelum ada peringkat
- Referat LakeslaDokumen36 halamanReferat Lakeslavenniariskia100% (1)
- Laporan Kasus PebDokumen38 halamanLaporan Kasus PebLili Suriani100% (1)
- Malaria PD Anak Dr. Irma SpADokumen52 halamanMalaria PD Anak Dr. Irma SpAelkana siringoringoBelum ada peringkat
- Referat Solusio PlasentaDokumen13 halamanReferat Solusio PlasentaalimustagialgiBelum ada peringkat
- Lapkas SepsisDokumen41 halamanLapkas SepsisramadhaniandaBelum ada peringkat
- SSCDokumen22 halamanSSCYulia Merita Sahdilla PutriBelum ada peringkat
- CASE GOUT FOME Fix Edit-DikonversiDokumen31 halamanCASE GOUT FOME Fix Edit-DikonversiWafya RamschieBelum ada peringkat
- Pedikulosis BSTDokumen23 halamanPedikulosis BSTWafya RamschieBelum ada peringkat
- Terapi Cairan RYANDokumen23 halamanTerapi Cairan RYANWafya RamschieBelum ada peringkat
- CRS TTHDokumen25 halamanCRS TTHWafya RamschieBelum ada peringkat
- TB WafyaDokumen8 halamanTB WafyaWafya RamschieBelum ada peringkat
- Crs HMFD, Wafy, EtilDokumen49 halamanCrs HMFD, Wafy, EtilWafya RamschieBelum ada peringkat
- Ilmiahnya DeviDokumen10 halamanIlmiahnya DeviWafya RamschieBelum ada peringkat
- PNPK Bedah Saraf 2016Dokumen285 halamanPNPK Bedah Saraf 2016komitemedik.rsudsda100% (1)
- Osce KPDDokumen10 halamanOsce KPDyuliasutotoBelum ada peringkat
- Referat DVTDokumen24 halamanReferat DVTnurul1102008296100% (4)
- Gizi BurukDokumen15 halamanGizi BurukWafya RamschieBelum ada peringkat
- CRS Total AV BlockDokumen25 halamanCRS Total AV BlockdennidililahariBelum ada peringkat
- Kabin GizburDokumen51 halamanKabin GizburWafya RamschieBelum ada peringkat
- HFMD FomeDokumen10 halamanHFMD FomeWafya RamschieBelum ada peringkat
- 55-Article Text-95-1-10-20171023Dokumen9 halaman55-Article Text-95-1-10-20171023farhanomeBelum ada peringkat
- CRS Total AV BlockDokumen25 halamanCRS Total AV BlockdennidililahariBelum ada peringkat
- Anemia Hemolitik Autoimun Laporan KasusDokumen31 halamanAnemia Hemolitik Autoimun Laporan KasusWafya RamschieBelum ada peringkat
- MH CaseDokumen37 halamanMH CaseWafya RamschieBelum ada peringkat
- Hal 46-55 No.2 Vol 25 2001. Trombosis Vena Dalam - IsiDokumen10 halamanHal 46-55 No.2 Vol 25 2001. Trombosis Vena Dalam - Isizano_adamBelum ada peringkat
- Matrik RPK Dan Ruk 2017Dokumen48 halamanMatrik RPK Dan Ruk 2017Wafya RamschieBelum ada peringkat
- Presentasi Rinitis AlergiDokumen53 halamanPresentasi Rinitis AlergiWafya RamschieBelum ada peringkat
- Crs Myoperikarditis - Wafy EditDokumen17 halamanCrs Myoperikarditis - Wafy EditWafya RamschieBelum ada peringkat
- Depresi Post PartumDokumen21 halamanDepresi Post PartumWafya RamschieBelum ada peringkat
- Tinjauan Pustaka SH-1Dokumen17 halamanTinjauan Pustaka SH-1Wafya RamschieBelum ada peringkat
- Journal Reading SjsDokumen19 halamanJournal Reading SjsWafya RamschieBelum ada peringkat
- Tinjauan Pustaka SH-1Dokumen17 halamanTinjauan Pustaka SH-1Wafya RamschieBelum ada peringkat
- AIHA Case ReportDokumen38 halamanAIHA Case ReportWafya RamschieBelum ada peringkat
- AIHA Case ReportDokumen38 halamanAIHA Case ReportWafya RamschieBelum ada peringkat
- AIHADokumen6 halamanAIHAAndik SubagiyoBelum ada peringkat