Anda mungkin juga menyukai
- Patofisiologi Infeksi Cacing - Rauza (2020)Dokumen52 halamanPatofisiologi Infeksi Cacing - Rauza (2020)Effika YuliaBelum ada peringkat
- ParotitisDokumen21 halamanParotitisRizKyImanSariBelum ada peringkat
- Inversio Uteri IfaDokumen25 halamanInversio Uteri IfaIfa MarlinaBelum ada peringkat
- Parasitologi UsusDokumen60 halamanParasitologi UsusCurie_JkBelum ada peringkat
- MEASLES ETIOLOGYDokumen27 halamanMEASLES ETIOLOGYTessalonichaBelum ada peringkat
- Tatalaksana DBDDokumen56 halamanTatalaksana DBDpuskesmas welahan2Belum ada peringkat
- Rupture Uretra Dan Buli-Buli - Putu Chika RadeantyDokumen33 halamanRupture Uretra Dan Buli-Buli - Putu Chika Radeantychika deantyBelum ada peringkat
- 1 Infeksi Salurah Kemih (Striktur Urethra Dan Prostatitis)Dokumen22 halaman1 Infeksi Salurah Kemih (Striktur Urethra Dan Prostatitis)marlisaBelum ada peringkat
- HIPOSPADIA & EPISPADIA REPAIRDokumen30 halamanHIPOSPADIA & EPISPADIA REPAIRDini YulidarBelum ada peringkat
- ISK GINJALDokumen49 halamanISK GINJALNoahYudhaBelum ada peringkat
- Varikokel, Hidrokel, Undesesus Testis, OrkhitisDokumen45 halamanVarikokel, Hidrokel, Undesesus Testis, OrkhitisRiki Muhadinul ikhsanBelum ada peringkat
- Nasogastric Suction Pada Dewasa (4A)Dokumen5 halamanNasogastric Suction Pada Dewasa (4A)Forza JuveBelum ada peringkat
- ANATOMI KULITDokumen47 halamanANATOMI KULITAgung Gek SandraBelum ada peringkat
- KUSTADokumen44 halamanKUSTASuci Sylvana HrpBelum ada peringkat
- Undescended TestisDokumen33 halamanUndescended TestisBobby SutojoBelum ada peringkat
- Penyebaran dan Daur Hidup Malaria di IndonesiaDokumen72 halamanPenyebaran dan Daur Hidup Malaria di IndonesiaNinda PangestikaBelum ada peringkat
- Bayi Post-Matur (3A)Dokumen6 halamanBayi Post-Matur (3A)Forza JuveBelum ada peringkat
- REKTAL TOUCHDokumen2 halamanREKTAL TOUCHIki IdriansyahBelum ada peringkat
- ENDOMETRITIS Dr. JMDokumen11 halamanENDOMETRITIS Dr. JMLam NandaBelum ada peringkat
- Salpingitis StationDokumen5 halamanSalpingitis StationuyauyaBelum ada peringkat
- EsofagitisDokumen30 halamanEsofagitisgreenluvBelum ada peringkat
- IMS dan HIV/AIDSDokumen65 halamanIMS dan HIV/AIDSIsmaryani Hazairin100% (1)
- CPR STATIONDokumen4 halamanCPR STATIONNorma Hanifah SBelum ada peringkat
- SOAL OSCE EMERGENCY DM TDK TerkontrolDokumen8 halamanSOAL OSCE EMERGENCY DM TDK Terkontroldanang bayuaji pratamaBelum ada peringkat
- Pembahasan UKDI KLINIK 1 Batch Ags 15 PDFDokumen440 halamanPembahasan UKDI KLINIK 1 Batch Ags 15 PDFakbar faerusBelum ada peringkat
- SchistosomiasisDokumen5 halamanSchistosomiasisNadya Lisfriana Novita IkasariBelum ada peringkat
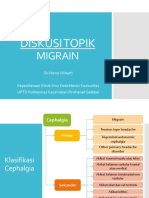
- DISKUSI TOPIK MigrainDokumen19 halamanDISKUSI TOPIK MigrainSri Nowo MinartiBelum ada peringkat
- Disentri ShigellosisDokumen23 halamanDisentri ShigellosisNatasya HerinBelum ada peringkat
- DispepsiaDokumen100 halamanDispepsiaIhsan HaidarBelum ada peringkat
- Tatalaksana Infeksi DengueDokumen52 halamanTatalaksana Infeksi DengueDyeriklilingBelum ada peringkat
- Soal OSCE DHF PediatriDokumen3 halamanSoal OSCE DHF Pediatripdureg_2012Belum ada peringkat
- DETEKSI DINI KANKER PROSTATDokumen19 halamanDETEKSI DINI KANKER PROSTATtaufiktayaBelum ada peringkat
- Dr. Richie S - MigrainDokumen25 halamanDr. Richie S - MigrainAnonymous FC99BLBelum ada peringkat
- OSCE DeliriumDokumen3 halamanOSCE DeliriumAnonymous l3X3jf0NPBelum ada peringkat
- Untuk menegakkan diagnosis dan manajemen yang tepat, saya usulkan pemeriksaan darah tepi untuk menilai kadar hemoglobin dan leukositDokumen56 halamanUntuk menegakkan diagnosis dan manajemen yang tepat, saya usulkan pemeriksaan darah tepi untuk menilai kadar hemoglobin dan leukositMuh Rizal AkhyarBelum ada peringkat
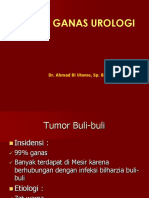
- KANKER UROLOGIDokumen88 halamanKANKER UROLOGIAri BetetBelum ada peringkat
- 3.1.2.2 Infeksi Saluran Kemih DewasaDokumen32 halaman3.1.2.2 Infeksi Saluran Kemih Dewasafaridatul lutfiBelum ada peringkat
- CSS PPT Dean Grestama SchistosomiasisDokumen14 halamanCSS PPT Dean Grestama SchistosomiasisDeanGrestamaBelum ada peringkat
- Aprinsip Pemeriksaan Patologi AnatomiDokumen68 halamanAprinsip Pemeriksaan Patologi AnatomiDara Fitri ShafiraBelum ada peringkat
- Case DHF - Zusmitha Desy PutriDokumen49 halamanCase DHF - Zusmitha Desy Putriraihan affandiBelum ada peringkat
- HYPOSPADIADokumen20 halamanHYPOSPADIA085241726591Belum ada peringkat
- Osce Nasional Feb 2015 MalariaDokumen7 halamanOsce Nasional Feb 2015 Malariamuhammadsukma30Belum ada peringkat
- Fistula UmbilikalisDokumen14 halamanFistula UmbilikalisaudyaBelum ada peringkat
- Gangguan SomatoformDokumen51 halamanGangguan Somatoformikhlasia AmaliBelum ada peringkat
- Pture Urethra, Rupture VUDokumen23 halamanPture Urethra, Rupture VUmelatiBelum ada peringkat
- 03 PreeklampsiaDokumen39 halaman03 PreeklampsiaRia Raissa FalaBelum ada peringkat
- KustaDokumen35 halamanKustaSofwatul 'Opan Ocay' AnamBelum ada peringkat
- VARIKOKELDokumen23 halamanVARIKOKELAdhelia Kusuma WardhaniBelum ada peringkat
- Tugas Presus - Habib Laksmana Prima - G4A019024 - Hidradenitis SuppurativaDokumen12 halamanTugas Presus - Habib Laksmana Prima - G4A019024 - Hidradenitis SuppurativaHabib LaksmanaBelum ada peringkat
- Template Osce StationDokumen5 halamanTemplate Osce StationVictor NainggolanBelum ada peringkat
- Bismillahirrahmanirrahim PPT Referat Lobus Oksipital Dan Batang Otak Dan CerebellumDokumen39 halamanBismillahirrahmanirrahim PPT Referat Lobus Oksipital Dan Batang Otak Dan Cerebellumaisyah100% (1)
- UROLITHIASISDokumen55 halamanUROLITHIASISIkramullah MahmuddinBelum ada peringkat
- Referat Sa'adahDokumen31 halamanReferat Sa'adah6130015051 MOHAMMAD QOIMAM BILQISTHI ZULFIKARBelum ada peringkat
- Isk - Dwi - FinalDokumen35 halamanIsk - Dwi - FinalNovitha DestaryBelum ada peringkat
- ISK BERULANGDokumen32 halamanISK BERULANGNovita Rotua Sari SitumeangBelum ada peringkat
- Css IskDokumen37 halamanCss IskFebrian AlfaroBelum ada peringkat
- Referat Infeksi Saluran KemihDokumen18 halamanReferat Infeksi Saluran KemihFerdita RidhaBelum ada peringkat
- 03 Cempaka Infeksi Saluran KemihDokumen17 halaman03 Cempaka Infeksi Saluran KemihRiaa RianaBelum ada peringkat
- Infeksi Saluran KemihDokumen35 halamanInfeksi Saluran KemihNiken MaretaBelum ada peringkat
- Urinary Tract InfectionsDokumen10 halamanUrinary Tract InfectionssindyBelum ada peringkat
- Panduan TriaseDokumen6 halamanPanduan TriasemarlisaBelum ada peringkat
- SK Pengkajian Awal KlinisDokumen2 halamanSK Pengkajian Awal KlinismarlisaBelum ada peringkat
- Osce SadanisDokumen2 halamanOsce SadanismarlisaBelum ada peringkat
- NOTULENSIDokumen1 halamanNOTULENSImarlisaBelum ada peringkat
- Osce IvaDokumen2 halamanOsce IvaAgustin Dwi UtamiBelum ada peringkat
- ISK-dr. Omega Kuliah ISK Modul 6.2 April 2020Dokumen49 halamanISK-dr. Omega Kuliah ISK Modul 6.2 April 2020marlisaBelum ada peringkat
- Invaginasi PDFDokumen7 halamanInvaginasi PDFMarlitaAdelinaBelum ada peringkat
- 1 Infeksi Salurah Kemih (Striktur Urethra Dan Prostatitis)Dokumen22 halaman1 Infeksi Salurah Kemih (Striktur Urethra Dan Prostatitis)marlisaBelum ada peringkat
- Form IvaDokumen14 halamanForm IvamarlisaBelum ada peringkat
- Materi Prof Aryati PDFDokumen13 halamanMateri Prof Aryati PDFMoch Alfian Arif DarmawanBelum ada peringkat
- Pengumuman Persiapan SKBDokumen3 halamanPengumuman Persiapan SKBmarlisaBelum ada peringkat
- Lampiran I Pengumuman SKBDokumen35 halamanLampiran I Pengumuman SKBmarlisaBelum ada peringkat
- elemen-penilaian-hand-hygieneDokumen2 halamanelemen-penilaian-hand-hygienemarlisaBelum ada peringkat
- Panduan Keterampilan Membaca Foto X'ray Skull & LumbosacralDokumen6 halamanPanduan Keterampilan Membaca Foto X'ray Skull & LumbosacralBrantBelum ada peringkat
- CARA PEMERIKSAAN JANTUNG DAN PEMBULUH DARAHDokumen44 halamanCARA PEMERIKSAAN JANTUNG DAN PEMBULUH DARAHUmero Syarif Al JufriBelum ada peringkat
- Panduan Manual Verifikasi Klaim Ina-Cbg: Edisi 1Dokumen69 halamanPanduan Manual Verifikasi Klaim Ina-Cbg: Edisi 1Matin Abdillah GogaBelum ada peringkat
- RADIOLOGIDokumen81 halamanRADIOLOGITri FebriastiBelum ada peringkat
- EKG Cara BacaDokumen23 halamanEKG Cara BacamarlisaBelum ada peringkat
- Dekontaminasi Cairan DarahDokumen2 halamanDekontaminasi Cairan DarahmarlisaBelum ada peringkat
- Soal SKB CPNS 2019 Materi Pokok Soal SKB Dengan CAT Untuk Seleksi CPNS Kabupaten Rembang Formasi Tahun 2019Dokumen75 halamanSoal SKB CPNS 2019 Materi Pokok Soal SKB Dengan CAT Untuk Seleksi CPNS Kabupaten Rembang Formasi Tahun 2019marlisa100% (2)
- PanuDokumen15 halamanPanumulkihakam21Belum ada peringkat