Anda mungkin juga menyukai
- Laporan Tutorial Perkembangan Gigi SGD 2Dokumen17 halamanLaporan Tutorial Perkembangan Gigi SGD 2Marissa AzzahraBelum ada peringkat
- Skenario 3 Proses MenuaDokumen32 halamanSkenario 3 Proses MenuaMeryam Suvi Nur Fitria100% (1)
- Pemeriksaan LengkapDokumen16 halamanPemeriksaan LengkapkelasC FKGBelum ada peringkat
- Tugas Kelompok Ikga 2Dokumen12 halamanTugas Kelompok Ikga 2Yustica TampubolonBelum ada peringkat
- Penuaan Tulang AlveolarDokumen43 halamanPenuaan Tulang AlveolarIcha MuntheBelum ada peringkat
- Perawatan Saluran AkarDokumen14 halamanPerawatan Saluran AkarBenny WirawanBelum ada peringkat
- Faktor Risiko KariesDokumen19 halamanFaktor Risiko KariesKurnia ApriantiBelum ada peringkat
- Preparasi, Skillab Restorasi PDFDokumen86 halamanPreparasi, Skillab Restorasi PDFPipitKusumaBelum ada peringkat
- GLAUKOMA AKUTDokumen25 halamanGLAUKOMA AKUTMentari AlishaBelum ada peringkat
- Penatalaksanaan Urtikaria Akut di Rongga MulutDokumen15 halamanPenatalaksanaan Urtikaria Akut di Rongga MulutAnonymous 8ab9VLKSqpBelum ada peringkat
- INFLAMASI GIGIDokumen24 halamanINFLAMASI GIGILuh Tu PebriyantiBelum ada peringkat
- Stomatitis Aftosa Rekuren Mayor FixDokumen9 halamanStomatitis Aftosa Rekuren Mayor FixMuhammad EffrinBelum ada peringkat
- Stomatitis Aphthous RecurrentDokumen3 halamanStomatitis Aphthous RecurrentAi Rafikah NurpratiwiBelum ada peringkat
- Radiologi Topik 5Dokumen48 halamanRadiologi Topik 5fevyliyadiBelum ada peringkat
- OdontoameloblastomaDokumen4 halamanOdontoameloblastomaanisa regitasariBelum ada peringkat
- Gejala Dan Tanda Awal Karies GigiDokumen1 halamanGejala Dan Tanda Awal Karies GigirevanvictoryBelum ada peringkat
- Prinsip, Pusat, Arah Tumbuh Kembang OrokraniofasialDokumen25 halamanPrinsip, Pusat, Arah Tumbuh Kembang OrokraniofasialnajlaBelum ada peringkat
- Tugas DRG - Silvia BAHAN BONDINGDokumen6 halamanTugas DRG - Silvia BAHAN BONDINGlolytofarisaBelum ada peringkat
- Laporan Sken 3 Alloy FixDokumen27 halamanLaporan Sken 3 Alloy FixGinanjar HidayatullahBelum ada peringkat
- Ameloblastic Fibro-Odontoma Pada Gadis 14 TahunDokumen4 halamanAmeloblastic Fibro-Odontoma Pada Gadis 14 TahunRenaldy ZMHPBelum ada peringkat
- ASAS KEDOKTERANDokumen6 halamanASAS KEDOKTERANAnonymous wsqCrNoeBelum ada peringkat
- Docshare - Tips - DSP 5 Amalgam Tattoo PDFDokumen18 halamanDocshare - Tips - DSP 5 Amalgam Tattoo PDFAyu SawitriBelum ada peringkat
- Lesi UlseratifDokumen8 halamanLesi UlseratifGita Putri KencanaBelum ada peringkat
- Laporan Tutorial Skenario 2Dokumen36 halamanLaporan Tutorial Skenario 2radin ahmadBelum ada peringkat
- Pemicu 1 - Blok 21 - Jeremias - 170600162Dokumen5 halamanPemicu 1 - Blok 21 - Jeremias - 170600162jeremias L.toruanBelum ada peringkat
- Klasifikasi Bahan CetakDokumen4 halamanKlasifikasi Bahan CetakVenesha SoniaBelum ada peringkat
- Stomatitis AlergikaDokumen22 halamanStomatitis AlergikaJeffrey PerryBelum ada peringkat
- KISTA RADIKULERDokumen4 halamanKISTA RADIKULER053 Komang Sri Anggita WijayantiBelum ada peringkat
- PERKEMBANGAN GIGIDokumen4 halamanPERKEMBANGAN GIGIDewiayu Shs DewangBelum ada peringkat
- KariesGigiDokumen5 halamanKariesGigiNia AprilitaBelum ada peringkat
- Perubahan Klinis Pada Rongga Mulut Akibat Proses PenuaanDokumen5 halamanPerubahan Klinis Pada Rongga Mulut Akibat Proses PenuaanZakiyya Ulpiyah100% (1)
- Mekanisme Menghindari Respon Host Oleh Bakteri Porphyromonas GingivalisDokumen2 halamanMekanisme Menghindari Respon Host Oleh Bakteri Porphyromonas GingivalisAngga NugrohoBelum ada peringkat
- 1-Struktur Jaringan PeriodontalDokumen30 halaman1-Struktur Jaringan PeriodontalMadinah ZainalBelum ada peringkat
- Trauma From OcclusionDokumen5 halamanTrauma From OcclusionRizalHendraKusumaBelum ada peringkat
- LI GVDokumen8 halamanLI GVAnonymous lVQhULbKcgBelum ada peringkat
- MIKROLEAKAGE PADA RESIN KOMPOSITDokumen10 halamanMIKROLEAKAGE PADA RESIN KOMPOSITnovetBelum ada peringkat
- UntitledDokumen14 halamanUntitledRhena Fitria KhairunnisaBelum ada peringkat
- Laporan Biokimia Cairan Rongga Mulut - Vania Aulia Nusanti - J2a021064Dokumen20 halamanLaporan Biokimia Cairan Rongga Mulut - Vania Aulia Nusanti - J2a021064vania auliaBelum ada peringkat
- Fase RemodelingDokumen3 halamanFase RemodelingPrabandityo TriwibowoBelum ada peringkat
- Faktor Predisposisi Terjadinya Penyakit PeriodontalDokumen9 halamanFaktor Predisposisi Terjadinya Penyakit PeriodontalSeptiana Putrining Suci AdiBelum ada peringkat
- PBL 2Dokumen3 halamanPBL 2Sannia SalsabilaBelum ada peringkat
- Pemeriksaan Intra OralDokumen3 halamanPemeriksaan Intra OralAditya ZulfikarBelum ada peringkat
- Diskusi 2 - KLAS 2 Amalgam Dan Klas 5 GICDokumen13 halamanDiskusi 2 - KLAS 2 Amalgam Dan Klas 5 GICDepiinaBelum ada peringkat
- Tutorial CBL BLOK 6Dokumen8 halamanTutorial CBL BLOK 6Ifata RDBelum ada peringkat
- Karies Dental dan Klasifikasi LesiDokumen6 halamanKaries Dental dan Klasifikasi LesiCynthia Anggraini PutriBelum ada peringkat
- Attachment PDFDokumen51 halamanAttachment PDFnuraeni296Belum ada peringkat
- BIBIRDokumen3 halamanBIBIRBestarikaBelum ada peringkat
- Inflamasi GingivaDokumen7 halamanInflamasi GingivaDhia ThifalBelum ada peringkat
- Impaksi GigiDokumen20 halamanImpaksi GigiAlexander RossBelum ada peringkat
- Skenario 2Dokumen25 halamanSkenario 2milhatulBelum ada peringkat
- P1 - Blok 9 - Brilianti Haditya - 190600088Dokumen16 halamanP1 - Blok 9 - Brilianti Haditya - 190600088Brilianti HadityaBelum ada peringkat
- Lesi Jaringan Lunak Rongga MulutDokumen13 halamanLesi Jaringan Lunak Rongga MulutRoza NafilahBelum ada peringkat
- Biokompatibilitas Bahan Kedokteran GigiDokumen1 halamanBiokompatibilitas Bahan Kedokteran GigiDewinta Candra PutriBelum ada peringkat
- KssDokumen0 halamanKssclaragustin_53768590Belum ada peringkat
- MOLEKULER GENETIKA OSTEOSARKOMADokumen24 halamanMOLEKULER GENETIKA OSTEOSARKOMAYanthie IndraBelum ada peringkat
- Kanker LidahDokumen17 halamanKanker LidahHanaMisakiBelum ada peringkat
- Tumor Esofagus dalamDokumen24 halamanTumor Esofagus dalamfan100% (1)
- SCC OralDokumen21 halamanSCC OralJanet UngBelum ada peringkat
- BAB 1 Kanker LidahDokumen14 halamanBAB 1 Kanker LidahFaiza Anak AliBelum ada peringkat
- Makalah Keperawatan Dewasa CA LidahDokumen21 halamanMakalah Keperawatan Dewasa CA LidahKristina RatihBelum ada peringkat
- Besten Mushroom IndustryDokumen39 halamanBesten Mushroom IndustryWiwin Nuril FalahBelum ada peringkat
- Defisiensi Vit DDokumen1 halamanDefisiensi Vit DMarisa PramasheillaBelum ada peringkat
- RundownDokumen2 halamanRundownWiwin Nuril FalahBelum ada peringkat
- Vit b12Dokumen1 halamanVit b12Wiwin Nuril FalahBelum ada peringkat
- Laporan CA IkgmDokumen6 halamanLaporan CA IkgmWiwin Nuril FalahBelum ada peringkat
- Ikga PPT FixDokumen14 halamanIkga PPT FixWiwin Nuril FalahBelum ada peringkat
- 3 Skripsi Pertiwi G0011157 2.6 IndDokumen16 halaman3 Skripsi Pertiwi G0011157 2.6 IndWiwin Nuril FalahBelum ada peringkat
- Rangkuman Banget NihDokumen2 halamanRangkuman Banget NihWiwin Nuril FalahBelum ada peringkat
- GingivitisDokumen8 halamanGingivitisWiwin Nuril FalahBelum ada peringkat
- Tata tertib kegiatanDokumen2 halamanTata tertib kegiatanWiwin Nuril FalahBelum ada peringkat
- Laporan Blok 3 SK 1Dokumen33 halamanLaporan Blok 3 SK 1Wiwin Nuril FalahBelum ada peringkat
- Laporan Blok 3 SK 1Dokumen29 halamanLaporan Blok 3 SK 1Wiwin Nuril FalahBelum ada peringkat
- What I Learned TodayDokumen6 halamanWhat I Learned TodayWiwin Nuril FalahBelum ada peringkat
- Penggunaan Fungsi If, Countif, LookupDokumen10 halamanPenggunaan Fungsi If, Countif, LookupYoga BotexBelum ada peringkat
- Peran PPKI Dalam Proses Persiapan Kemerdekaan IndonesiaDokumen2 halamanPeran PPKI Dalam Proses Persiapan Kemerdekaan IndonesiaWiwin Nuril Falah80% (5)
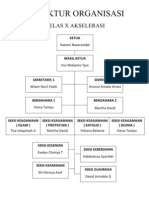
- Struktur Organisasi X AkselDokumen1 halamanStruktur Organisasi X AkselWiwin Nuril FalahBelum ada peringkat
- Fisiologi Saraf - Wiwin Nuril Falah 135070400111042Dokumen3 halamanFisiologi Saraf - Wiwin Nuril Falah 135070400111042Wiwin Nuril FalahBelum ada peringkat
- ListrikDokumen78 halamanListrikRatna Zakia HasmyBelum ada peringkat
- UjianakhirpenjasDokumen7 halamanUjianakhirpenjasWiwin Nuril FalahBelum ada peringkat